

Fatal outcome after insufficient spine fixation for pyogenic thoracic spondylodiscitis: an imperative for 360 degrees fusion of the infected spine
- PMID: 19243602
- PMCID: PMC2654872
- DOI: 10.1186/1754-9493-3-4
Fatal outcome after insufficient spine fixation for pyogenic thoracic spondylodiscitis: an imperative for 360 degrees fusion of the infected spine
Abstract
Background: Pyogenic spondylodiscitis represents a potentially life-threatening condition. Due to the low incidence, evidence-based surgical recommendations in the literature are equivocal, and the treatment modalities remain controversial.
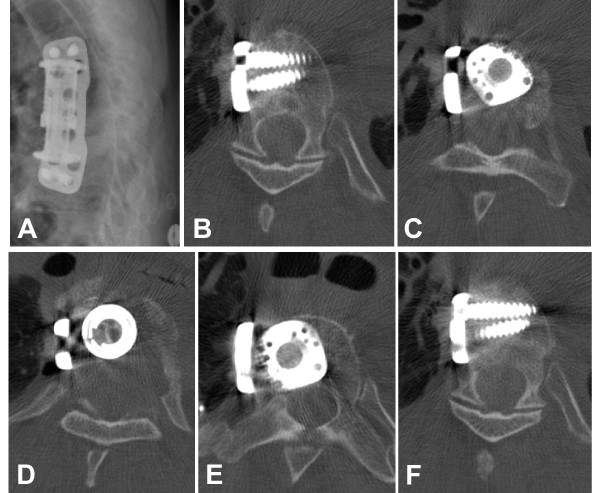
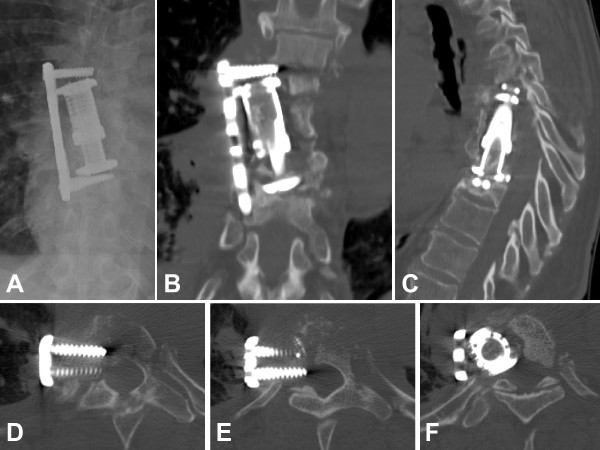
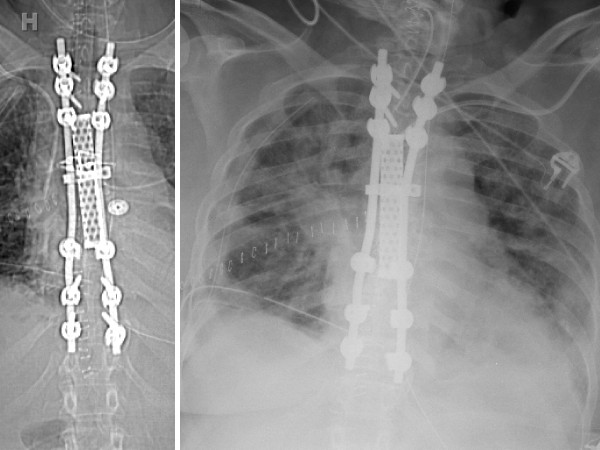
Case presentation: A 59 year-old patient presented with a history of thoracic spondylodiscitis resistant to antibiotic treatment for 6 weeks, progressive severe back pain, and a new onset of bilateral lower extremity weakness. Clinically, the patient showed a deteriorating spastic paraparesis of her lower extremities. An emergent MRI revealed a kyphotic wedge compression fracture at T7/T8 with significant spinal cord compression, paravertebral and epidural abscess, and signs of myelopathy. The patient underwent surgical debridement with stabilization of the anterior column from T6-T9 using an expandable titanium cage, autologous bone graft, and an anterolateral locking plate. The patient recovered well under adjunctive antibiotic treatment. She presented again to the emergency department 6 months later, secondary to a repeat fall, with acute paraplegia of the lower extremities and radiographic evidence of failure of fixation of the anterior T-spine. She underwent antero-posterior revision fixation with hardware removal, correction of kyphotic malunion, evacuation of a recurrent epidural abscess, decompression of the spinal canal, and 360 degrees fusion from T2-T11. Despite the successful salvage procedure, the patient deteriorated in the postoperative phase, when she developed multiple complications including pneumonia, acute respiratory distress syndrome, bacterial meningitis, abdominal compartment syndrome, followed by septic shock with multiple organ failure and a lethal outcome within two weeks after revision surgery.
Conclusion: This catastrophic example of a lethal outcome secondary to failure of anterior column fixation for pyogenic thoracic spondylodiscitis underlines the notion that surgical strategies for the infected spine must be aimed at achieving absolute stability by a 360 degrees fusion. This aggressive - albeit controversial - concept allows for an adequate infection control by adjunctive antibiotics and reduces the imminent risk of a secondary loss of fixation due to compromises in initial fixation techniques.
Figures

Similar articles
-
Hematogenous pyogenic spinal infections and their surgical management.Spine (Phila Pa 1976). 2000 Jul 1;25(13):1668-79. doi: 10.1097/00007632-200007010-00010. Spine (Phila Pa 1976). 2000. PMID: 10870142
-
Surgical results of long posterior fixation with short fusion in the treatment of pyogenic spondylodiscitis of the thoracic and lumbar spine: a retrospective study.Spine (Phila Pa 1976). 2012 Dec 1;37(25):E1572-9. doi: 10.1097/BRS.0b013e31827399b8. Spine (Phila Pa 1976). 2012. PMID: 22996263
-
Complete recovery of acute paraplegia due to pyogenic thoracic spondylodiscitis with an epidural abscess.Acta Neurochir (Wien). 2008 Apr;150(4):381-6. doi: 10.1007/s00701-007-1485-6. Epub 2008 Jan 8. Acta Neurochir (Wien). 2008. PMID: 18176773
-
Treatment of osteomyelitis of the spine using percutaneous suction/irrigation and percutaneous external spinal fixation.J Spinal Disord. 1994 Jun;7(3):185-205. doi: 10.1097/00002517-199407030-00001. J Spinal Disord. 1994. PMID: 7919642 Review.
-
Management of Postoperative Spondylodiscitis with and without Internal Fixation.Turk Neurosurg. 2015;25(4):513-8. doi: 10.5137/1019-5149.JTN.9008-13.1. Turk Neurosurg. 2015. PMID: 26242325 Review.
Cited by
-
Surgical Management of L5-S1 Spondylodiscitis on Previously Documented Isthmic Spondylolisthesis: Case Report and Review of the Literature.Case Rep Surg. 2020 Feb 15;2020:1408701. doi: 10.1155/2020/1408701. eCollection 2020. Case Rep Surg. 2020. PMID: 32128267 Free PMC article.
-
Single-stage debridement and spinal fusion using PEEK cages through a posterior approach for eradication of lumbar pyogenic spondylodiscitis: a safe treatment strategy for a detrimental condition.Patient Saf Surg. 2015 Nov 10;9:35. doi: 10.1186/s13037-015-0083-4. eCollection 2015. Patient Saf Surg. 2015. PMID: 26561500 Free PMC article.
-
Posterior only versus combined posterior and anterior approaches in surgical management of lumbosacral tuberculosis with paraspinal abscess in adults.Eur J Trauma Emerg Surg. 2014 Oct;40(5):607-16. doi: 10.1007/s00068-013-0367-2. Epub 2014 Jan 21. Eur J Trauma Emerg Surg. 2014. PMID: 26814519
-
360-degree cervical spinal arthrodesis for treatment of pediatric cervical spinal tuberculosis with kyphosis.BMC Musculoskelet Disord. 2016 Apr 23;17:175. doi: 10.1186/s12891-016-1034-7. BMC Musculoskelet Disord. 2016. PMID: 27108221 Free PMC article.
-
One-stage lumbopelvic fixation in the treatment of lumbosacral junction tuberculosis.Eur Spine J. 2015 Aug;24(8):1800-5. doi: 10.1007/s00586-015-3863-8. Epub 2015 Mar 11. Eur Spine J. 2015. PMID: 25757533
References
-
- Grammatico L, Besnier JM. Infectious spondylodiscitis. Rev Prat. 2007;57:970–978. - PubMed
-
- Danner RL, Hartman BJ. Update on spinal epidural abscess: 35 cases and review of the literature. Rev Infect Dis. 1987;9:265–274. - PubMed
-
- Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997;79:874–880. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
