

Co-morbidity and visual acuity are risk factors for health-related quality of life decline: five-month follow-up EQ-5D data of visually impaired older patients
- PMID: 19243624
- PMCID: PMC2654874
- DOI: 10.1186/1477-7525-7-18
Co-morbidity and visual acuity are risk factors for health-related quality of life decline: five-month follow-up EQ-5D data of visually impaired older patients
Abstract
Background: Co-morbidity is a common phenomenon in the elderly and is considered to be a major threat to quality of life (QOL). Knowledge of co-existing conditions or patient characteristics that lead to an increased QOL decline is important for individual care, and for public health purposes. In visually impaired older adults, it remains unclear which co-existing conditions or other characteristics influence their health-related QOL. Our aim was to present a risk profile of characteristics and conditions which predict deterioration of QOL in visually impaired older patients.
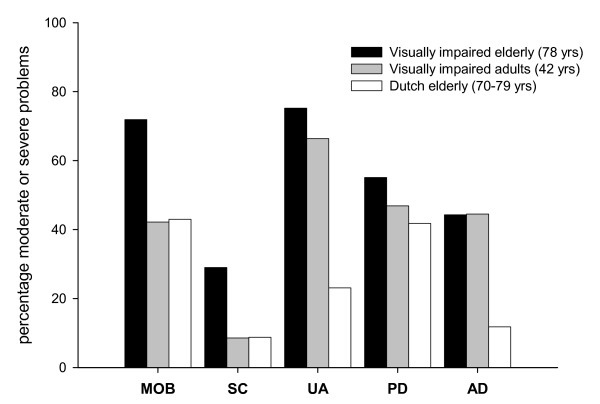
Methods: Analyses were performed on data from an observational study among 296 visually impaired older patients from four Dutch hospitals. QOL was measured with the EuroQol-5D (EQ-5D) at baseline and at five-month follow-up. Nine co-existing condition categories (musculoskeletal; diabetes; heart; hypertension; chronic obstructive pulmonary disease (COPD) or asthma; hearing impairment; stroke; cancer; gastrointestinal conditions) and six patient characteristics (age; gender; visual acuity; social status; independent living; rehabilitation type) were tested in a linear regression model to determine the risk profile. The model was corrected for baseline EQ-5D scores. In addition, baseline EQ-5D scores were compared with reference scores from a younger visually impaired population and from elderly in the general population.
Results: From the 296 patients, 50 (16.9%) were lost to follow-up. Patients who reported diabetes, COPD or asthma, consequences of stroke, musculoskeletal conditions, cancer, gastrointestinal conditions or higher logMAR Visual Acuity values, experienced a lower QOL. After five months, visual acuity, musculoskeletal conditions, COPD/asthma and stroke predicted a decline in QOL (R2 = 0.20). At baseline, the visually impaired older patients more often reported moderate or severe problems on most EQ-5D dimensions than the two reference groups.
Conclusion: In visually impaired older patients, visual acuity, musculoskeletal conditions, COPD/asthma and stroke predicted a relatively rapid decline in health-related QOL. With this risk profile, a specific referral by the ophthalmologist to another sub-specialty may have a beneficial effect on the patient's health-related QOL. A referral by the ophthalmologist or optometrist to a multidisciplinary rehabilitation service seems appropriate for some patients with co-morbidity. The current results need to be confirmed in studies using pre-structured questionnaires to assess co-morbidity.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
