

Correlation of MR imaging and MR spectroscopic imaging findings with Ki-67, phospho-Akt, and androgen receptor expression in prostate cancer
- PMID: 19244047
- PMCID: PMC2680166
- DOI: 10.1148/radiol.2503080473
Correlation of MR imaging and MR spectroscopic imaging findings with Ki-67, phospho-Akt, and androgen receptor expression in prostate cancer
Abstract
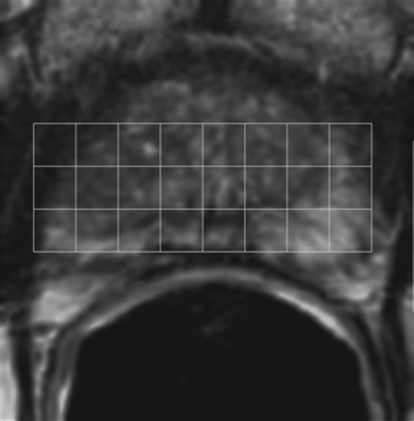
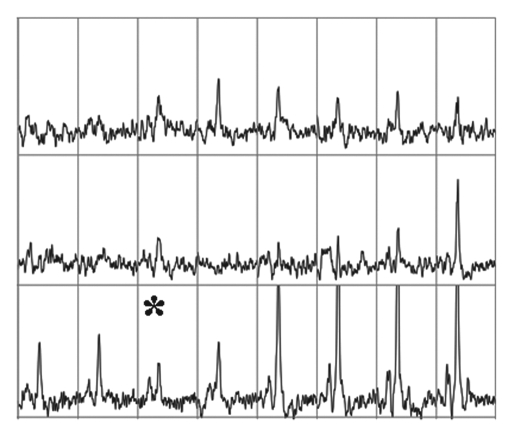
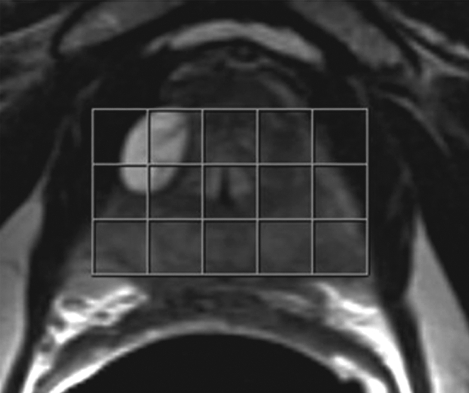
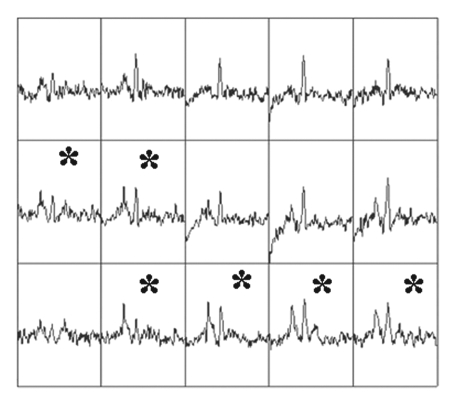
Purpose: To retrospectively assess whether magnetic resonance (MR) imaging and MR spectroscopic imaging and selected molecular markers correlate with each other and with clinically insignificant and significant prostate cancer (PCa), as defined at surgical pathologic analysis.
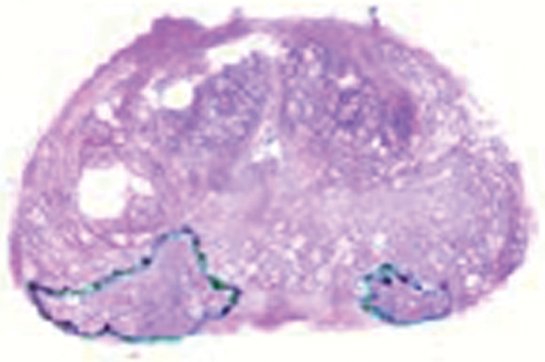
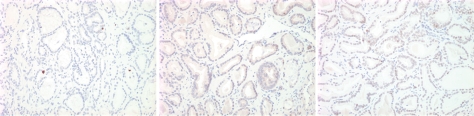
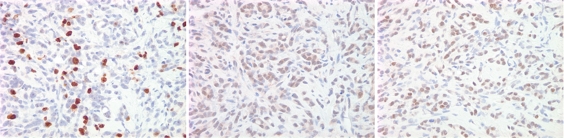
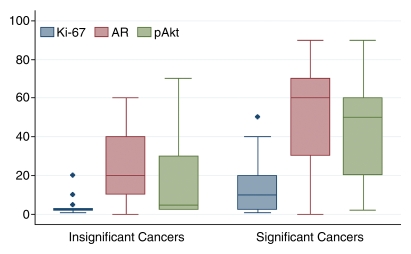
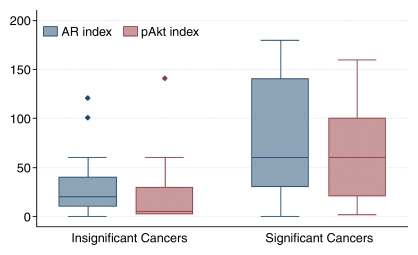
Materials and methods: The institutional review board approved this HIPAA-compliant study and waived informed consent. Eighty-nine men (mean age, 63 years; range, 46-79 years) with biopsy-proved PCa underwent combined endorectal MR imaging and MR spectroscopic imaging before radical prostatectomy. Suspicion of clinically insignificant PCa was retrospectively and separately recorded for MR imaging and combined MR imaging and MR spectroscopic imaging by using a scale of 0-3. Clinically insignificant PCa was pathologically defined as organ-confined cancer of 0.5 cm(3) or less without poorly differentiated elements. Prostatectomy specimens underwent immunohistochemical analysis for three molecular markers: Ki-67, phospho-Akt (pAkt), and androgen receptor (AR). To examine differences in marker levels for clinically insignificant and significant cancer, a Wilcoxon rank sum test was used. To examine correlations between marker levels and MR imaging or combined MR imaging and MR spectroscopic imaging scores, the Spearman correlation was used.
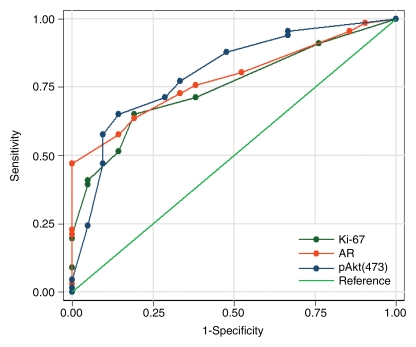
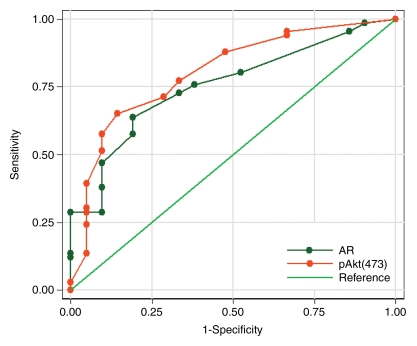
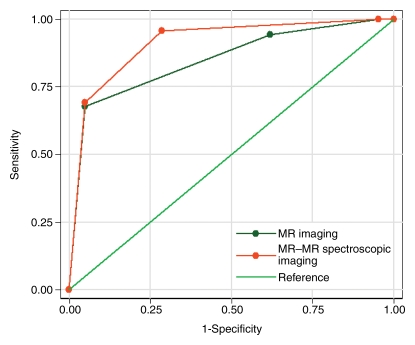
Results: Twenty-one (24%) patients had clinically insignificant and 68 (76%) had clinically significant PCa at surgical pathologic review. All markers were significantly correlated with MR imaging and combined MR imaging and MR spectroscopic imaging findings (all correlation coefficients >0.5). In differentiating clinically insignificant from clinically significant PCa, areas under the receiver operating characteristic curves for Ki-67, AR, pAkt, MR imaging, and combined MR imaging and MR spectroscopic imaging were 0.75, 0.78, 0.80, 0.85, and 0.91, respectively.
Conclusion: The use of pretreatment MR imaging or combined MR imaging and MR spectroscopic imaging and molecular marker analyses of biopsy samples could facilitate better treatment selection.
Supplemental material: http://radiology.rsnajnls.org/cgi/content/full/250/3/803/DC1.
RSNA, 2009
Figures

Similar articles
-
Prediction of prostate cancer recurrence using magnetic resonance imaging and molecular profiles.Clin Cancer Res. 2009 Jun 1;15(11):3842-9. doi: 10.1158/1078-0432.CCR-08-2453. Epub 2009 May 12. Clin Cancer Res. 2009. PMID: 19435838 Free PMC article.
-
Prostate cancer: identification with combined diffusion-weighted MR imaging and 3D 1H MR spectroscopic imaging--correlation with pathologic findings.Radiology. 2008 Feb;246(2):480-8. doi: 10.1148/radiol.2462070368. Radiology. 2008. PMID: 18227542
-
Clinical stage T1c prostate cancer: evaluation with endorectal MR imaging and MR spectroscopic imaging.Radiology. 2009 Nov;253(2):425-34. doi: 10.1148/radiol.2532081390. Radiology. 2009. PMID: 19864529 Free PMC article.
-
MR imaging and MR spectroscopic imaging of prostate cancer.Magn Reson Imaging Clin N Am. 2004 Aug;12(3):557-79, vii. doi: 10.1016/j.mric.2004.03.011. Magn Reson Imaging Clin N Am. 2004. PMID: 15271371 Review.
-
Multiparametric MRI in detection and staging of prostate cancer.Dan Med J. 2017 Feb;64(2):B5327. Dan Med J. 2017. PMID: 28157066 Review.
Cited by
-
Multi-kernel graph embedding for detection, Gleason grading of prostate cancer via MRI/MRS.Med Image Anal. 2013 Feb;17(2):219-35. doi: 10.1016/j.media.2012.10.004. Epub 2012 Dec 13. Med Image Anal. 2013. PMID: 23294985 Free PMC article.
-
A decade in prostate cancer: from NMR to metabolomics.Nat Rev Urol. 2011 May 17;8(6):301-11. doi: 10.1038/nrurol.2011.53. Nat Rev Urol. 2011. PMID: 21587223 Review.
-
The potential role of magnetic resonance spectroscopy in image-guided radiotherapy.Front Oncol. 2014 May 5;4:91. doi: 10.3389/fonc.2014.00091. eCollection 2014. Front Oncol. 2014. PMID: 24847443 Free PMC article. Review.
-
Physical passaging of embryoid bodies generated from human pluripotent stem cells.PLoS One. 2011 May 3;6(5):e19134. doi: 10.1371/journal.pone.0019134. PLoS One. 2011. PMID: 21559272 Free PMC article.
-
Computer-aided Detection of Prostate Cancer with MRI: Technology and Applications.Acad Radiol. 2016 Aug;23(8):1024-46. doi: 10.1016/j.acra.2016.03.010. Epub 2016 Apr 25. Acad Radiol. 2016. PMID: 27133005 Free PMC article. Review.
References
-
- Klein EA. What is ‘insignificant’ prostate carcinoma? Cancer 2004;101:1923–1925. - PubMed
-
- Epstein JI, Chan DW, Sokoll LJ, et al. Nonpalpable stage T1c prostate cancer: prediction of insignificant disease using free/total prostate specific antigen levels and needle biopsy findings. J Urol 1998;160:2407. - PubMed
-
- Epstein JI, Sanderson H, Carter HB, Scharfstein DO. Utility of saturation biopsy to predict insignificant cancer at radical prostatectomy. Urology 2005;66:356–360. - PubMed
-
- Epstein JI, Walsh PC, Carmichael M, Brendler CB. Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994;271:368–374. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
