

Review
doi: 10.1056/NEJMra0801454.
Preservation of fertility in patients with cancer
Affiliations
- PMID: 19246362
- PMCID: PMC2927217
- DOI: 10.1056/NEJMra0801454
Item in Clipboard
Review
Preservation of fertility in patients with cancer
N Engl J Med.
.
No abstract available
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
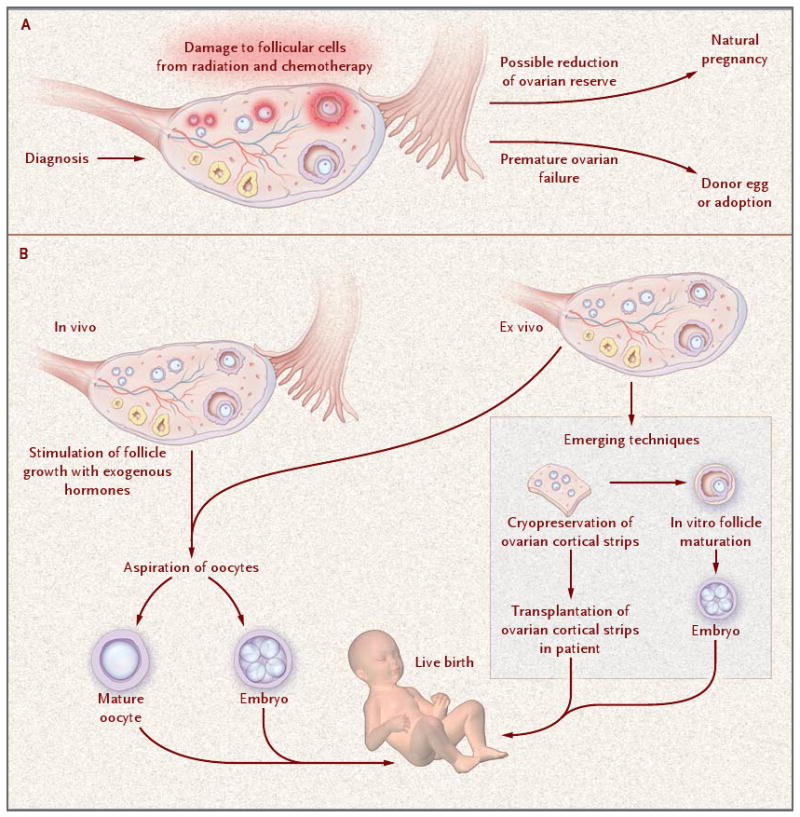
As shown in Panel A, high-dose radiation and most chemotherapeutic agents damage the growing cells in mature and immature follicles and, depending on the type of drug, the dose, and the age of the patient, may result in depletion of many or all follicles. This depletion may result in a short-term loss of reproductive function and an inability to attain a natural pregnancy after treatment. As shown in Panel B, if fertility interventions are warranted, the patient can delay treatment and undergo hormonal induction for 2 to 3 weeks to stimulate follicle development and recover mature oocytes. The oocytes can be frozen or fertilized, depending on the wishes of the patient. If there is insufficient time or if there are contraindications, one ovary can be removed, and ovarian cortical strips can be cryopreserved for use in tissue transplantation or emerging techniques such as in vitro follicle maturation.
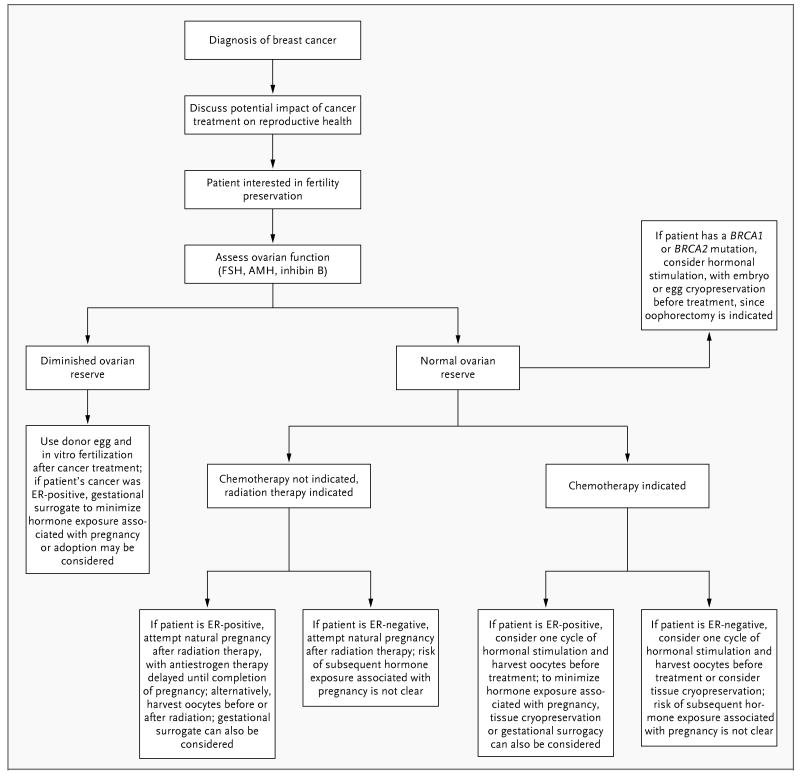
A discussion about the threat treatment poses to fertility is a critical part of the care of young patients with cancer, in order to allay concerns or offer options for preserving fertility. Some patients may have baseline infertility (i.e., infertility that is independent of the disease), and patients with recurrent disease may have diminished ovarian reserve as a result of previous chemotherapy. The clinician can determine the premenopausal status of the patient by asking about the menstrual history and obtaining a measurement of the follicle-stimulating hormone (FSH) level; an elevated level on an early day in the menstrual cycle indicates diminished ovarian reserve. Strategies for preserving fertility are then established, depending on treatment decisions and the time available for intervention. A multidisciplinary team that provides advice on these cases can help ensure that the complex decisions made by the clinician and the patient are integrated and that risk–benefit discussions about all decisions are clearly delineated. AMH denotes antimüllerian hormone, and ER estrogen receptor.
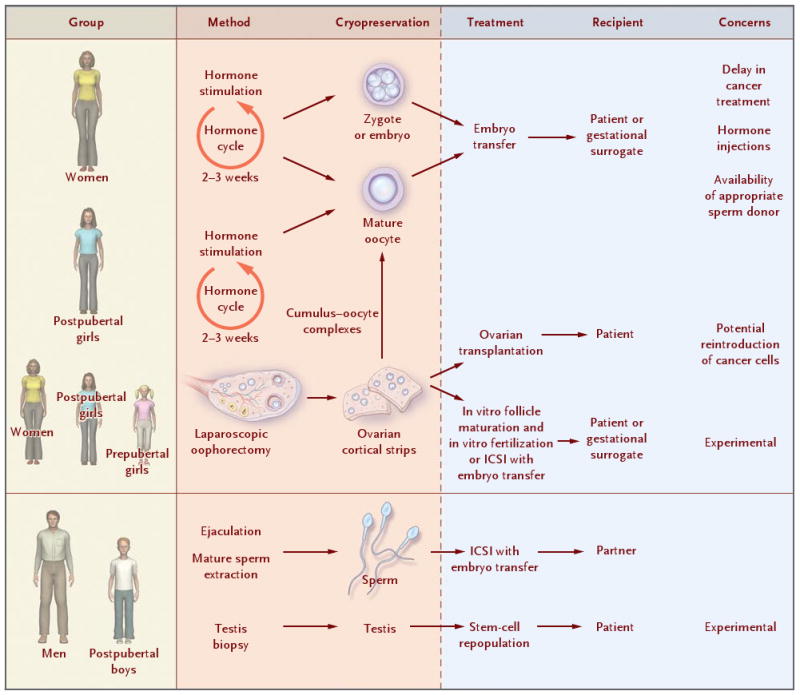
Fertility-preserving options for young women with cancer include hormonal stimulation with cryopreservation of oocytes or embryos and laparoscopic oophorectomy with tissue storage and later use in transplantation or in vitro follicle maturation. At the time of tissue harvest, mature follicles may exist and cumulus–oocyte complexes may be harvested and matured in vitro to provide another source of mature eggs for storage. Depending on the patient's uterine status, a gestational surrogate may be required. Tissue cryopreservation is the only option for girls who are not candidates for hormone stimulation. Cryopreservation of ejaculatory or tissue-extracted sperm is an option in men and postpubertal boys with cancer. ICSI denotes intracytoplasmic sperm injection.
Comment in
-
Preservation of fertility in patients with cancer.N Engl J Med. 2009 Jun 18;360(25):2680; author reply 2682-3. doi: 10.1056/NEJMc090614. N Engl J Med. 2009. PMID: 19535811 No abstract available.
-
Preservation of fertility in patients with cancer.N Engl J Med. 2009 Jun 18;360(25):2680-1; author reply 2682-3. N Engl J Med. 2009. PMID: 19537322 No abstract available.
-
Preservation of fertility in patients with cancer.N Engl J Med. 2009 Jun 18;360(25):2681-2; author reply 2682-3. N Engl J Med. 2009. PMID: 19537323 No abstract available.
-
Preservation of fertility in patients with cancer.N Engl J Med. 2009 Jun 18;360(25):2681; author reply 2682-3. N Engl J Med. 2009. PMID: 19537324 No abstract available.
-
Preservation of fertility in patients with cancer.N Engl J Med. 2009 Jun 18;360(25):2682; author reply 2682-3. N Engl J Med. 2009. PMID: 19537325 No abstract available.
References
-
- Woodruff TK. The emergence of a new interdiscipline: oncofertility. Cancer Treat Res. 2007;138:3–11. - PubMed
-
- Agarwal SK, Chang RJ. Fertility management for women with cancer. Cancer Treat Res. 2007;138:15–27. - PubMed
-
- Donaldson SS, Link MP, Weinstein HJ, et al. Final results of a prospective clinical trial with VAMP and low-dose involved-field radiation for children with low-risk Hodgkin's disease. J Clin Oncol. 2007;25:332–7. - PubMed
-
- Hayes DF, Thor AD, Dressler LG, et al. HER2 and response to paclitaxel in nodepositive breast cancer. N Engl J Med. 2007;357:1496–506. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical