

Intraventricular hemorrhage: severity factor and treatment target in spontaneous intracerebral hemorrhage
- PMID: 19246695
- PMCID: PMC2744212
- DOI: 10.1161/STROKEAHA.108.535419
Intraventricular hemorrhage: severity factor and treatment target in spontaneous intracerebral hemorrhage
Abstract
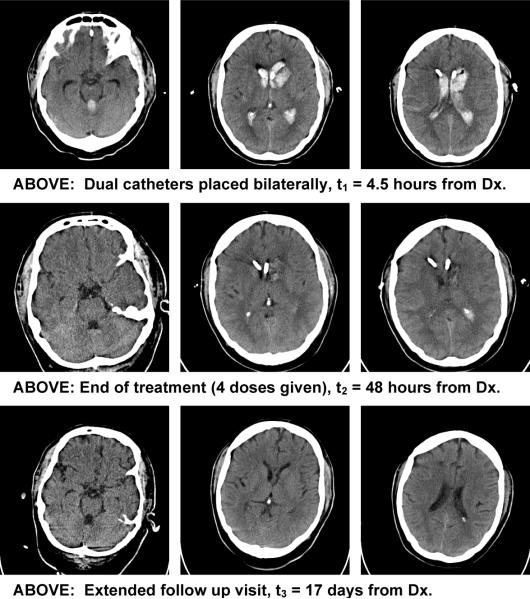
Background and purpose: This review focuses on the emerging principles of intracerebral hemorrhage (ICH) management, emphasizing the natural history and treatment of intraventricular hemorrhage. The translational and clinical findings from recent randomized clinical trials are defined and discussed. Summary of Review- Brain hemorrhage is the most severe of the major stroke subtypes. Extension of the hemorrhage into the ventricles (a 40% occurrence) can happen early or late in the sequence of events. Epidemiological data demonstrate the amount of blood in the ventricles relates directly to the degree of injury and likelihood of survival. Secondary tissue injury processes related to intraventricular bleeding can be reversed by removal of clot in animals. Specific benefits of removal include limitation of inflammation, edema, and cell death, as well as restoration of cerebral spinal fluid flow, intracranial pressure homeostasis, improved consciousness, and shortening of intensive care unit stay. Limited clinical knowledge exists about the benefits of intraventricular hemorrhage (IVH) removal in humans, because organized attempts to remove blood have not been undertaken in large clinical trials on a generalized scale. New tools to evaluate the volume and location of IVH and to test the benefits/risks of removal have been used in the clinical domain. Initial efforts are encouraging that increased survival and functional improvement can be achieved. Little controversy exists regarding the need to scientifically investigate treatment of this severity factor.
Conclusions: Animal models demonstrate clot removal can improve the acute and long-term consequences of intraventricular extension from intracerebral hemorrhage by using minimally invasive techniques coupled to recombinant tissue plasminogen activator-mediated clot lysis. The most recent human clinical trials show that severity of initial injury and the long-term consequences of blood extending into the ventricles are clearly related to the amount of bleeding into the ventricular system. The failure of the last 2 pivotal brain hemorrhage randomized control trials may well relate to the consequences of intraventricular bleeding. Small proof of concept studies, meta-analyses, and preliminary pharmacokinetics studies support the idea of positive shifts in mortality and morbidity, if this 1 critical disease severity factor, IVH, is properly addressed. Understanding clinical methods for the removal of IVH is required if survival and long-term functional outcome of brain hemorrhage is to improve worldwide.
Figures
References
-
- Teernstra OP, Evers SM, Kessels AH. Meta analyses in treatment of spontaneous supratentorial intracerebral haematoma. Acta Neurochir (Wien) 2006;148:521–528. discussion 528. - PubMed
-
- Dennis MS. Outcome after brain haemorrhage. Cerebrovasc Dis. 2003;16:9–13. - PubMed
-
- Lovelock CE, Molyneux AJ, Rothwell PM. Change in incidence and aetiology of intracerebral haemorrhage in oxfordshire, uk, between 1981 and 2006: A population-based study. Lancet Neurol. 2007;6:487–493. - PubMed
-
- Xi G, Keep FR, Hoff JT. Pathophysiology of brain edema formation. Neurosurg Clin N Am. 2002;13:371–383. - PubMed
-
- Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, Shaw MD, Barer DH, Investigators S. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the international surgical trial in intracerebral haemorrhage (stich): A randomised trial. Lancet. 2005;365:387–397. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
