

Global genomic analysis of intraductal papillary mucinous neoplasms of the pancreas reveals significant molecular differences compared to ductal adenocarcinoma
- PMID: 19247032
- PMCID: PMC3957431
- DOI: 10.1097/SLA.0b013e31819a6e16
Global genomic analysis of intraductal papillary mucinous neoplasms of the pancreas reveals significant molecular differences compared to ductal adenocarcinoma
Abstract
Objective: To determine whether intraductal papillary mucinous neoplasms of the pancreas (IPMNs) have a different genetic background compared with ductal adenocarcinoma (PDAC).
Summary background data: The biologic and clinical behavior of IPMNs and IPMN-associated adenocarcinomas is different from PDAC in having a less aggressive tumor growth and significantly improved survival. Up to date, the molecular mechanisms underlying the clinical behavior of IPMNs are incompletely understood.
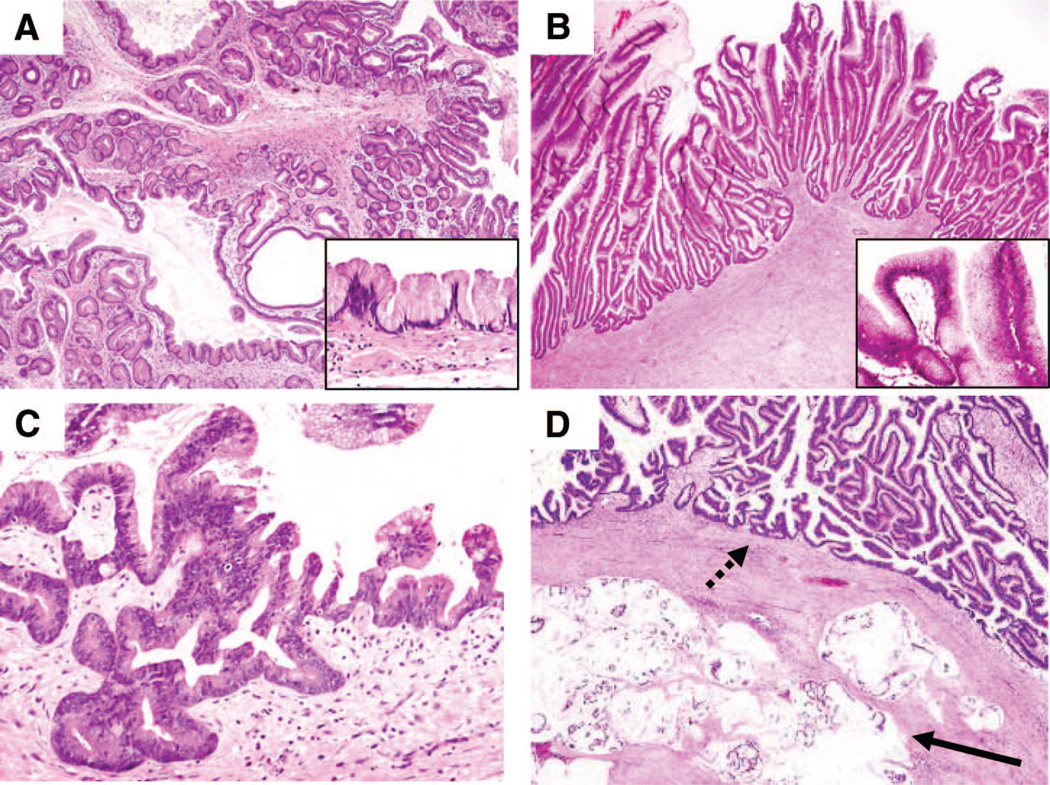
Methods: 128 cystic pancreatic lesions were prospectively identified during the course of 2 years. From the corresponding surgical specimens, 57 IPMNs were separated and subdivided by histologic criteria into those with low-grade dysplasia, moderate dysplasia, high-grade dysplasia, and invasive cancer. Twenty specimens were suitable for DNA isolation and subsequent performance of array CGH.
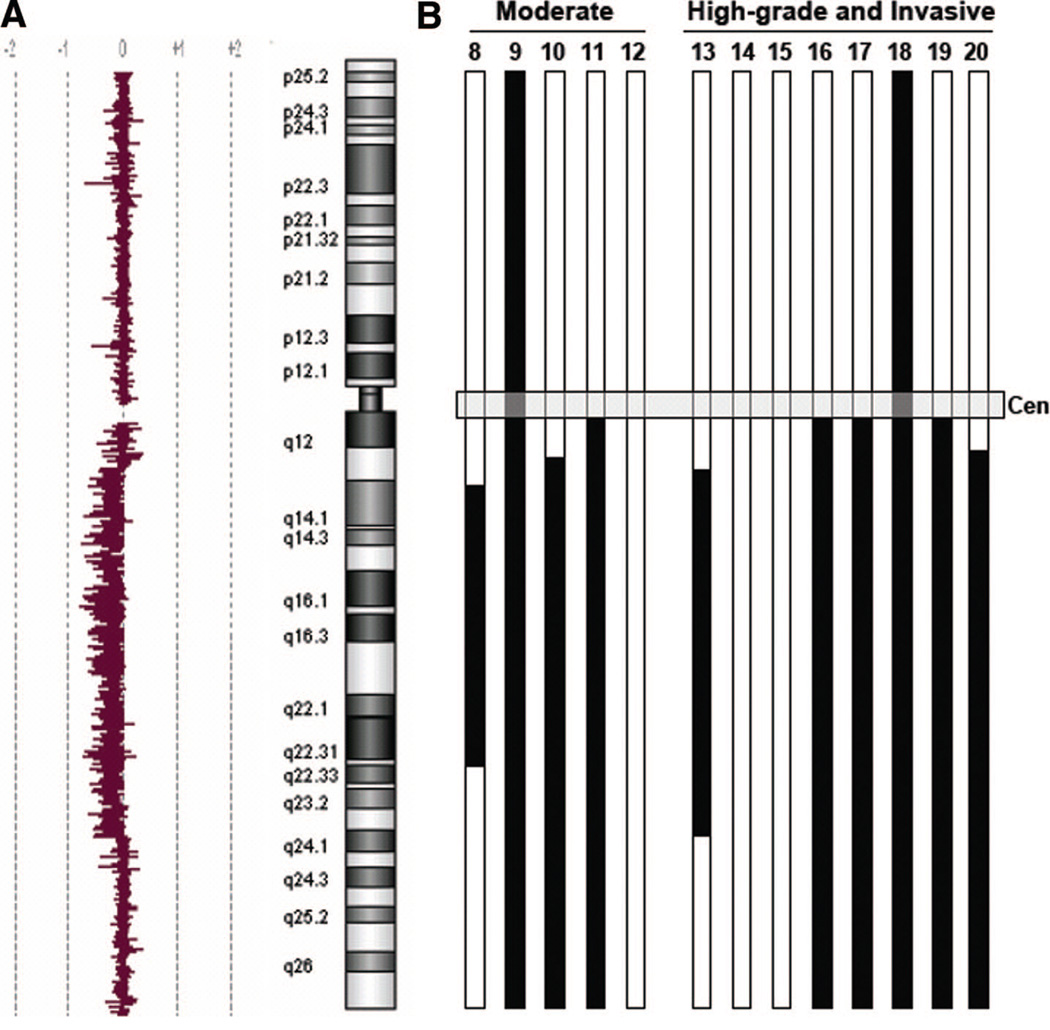
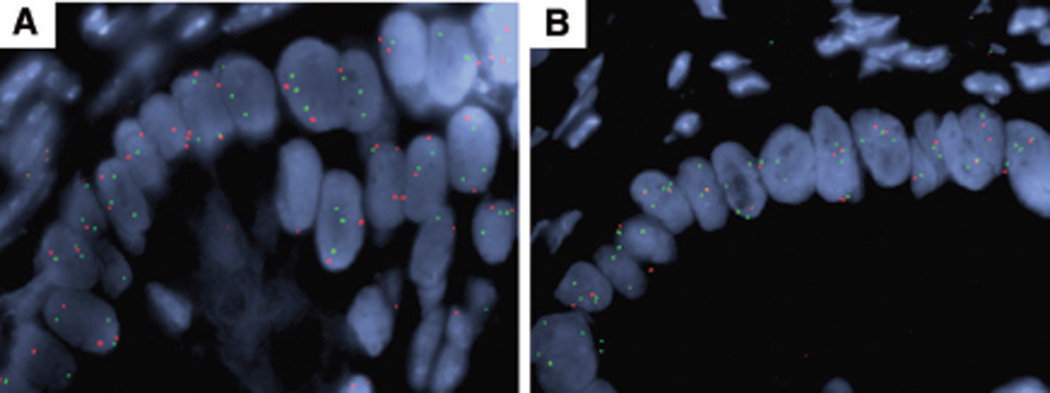
Results: While none of the IPMNs with low-grade dysplasia displayed detectable chromosomal aberrations, IPMNs with moderate and high-grade dysplasia showed frequent copy number alterations. Commonly lost regions were located on chromosome 5q, 6q, 10q, 11q, 13q, 18q, and 22q. The incidence of loss of chromosome 5q, 6q, and 11q was significantly higher in IPMNs with high-grade dysplasia or invasion compared with PDAC. Ten of 13 IPMNs with moderate dysplasia or malignancy had loss of part or all of chromosome 6q, with a minimal deleted region between linear positions 78.0 and 130.0.
Conclusions: This study is the first to use array CGH to characterize IPMNs. Recurrent cytogenetic alterations were identified and were different than those described in PDAC. Array CGH may help distinguish between these 2 entities and give insight into the differences in their biology and prognosis.
Conflict of interest statement
Conflict of Interest: The authors report no conflicts of interest.
Figures
References
-
- Conlon KC. Intraductal papillary mucinous tumors of the pancreas. J Clin Oncol. 2005;23(20):4518–4523. - PubMed
-
- Sarr MG, Murr M, Smyrk TC, et al. Primary cystic neoplasms of the pancreas. Neoplastic disorders of emerging importance-current state-of-the-art and unanswered questions. J Gastrointest Surg. 2003;7(3):417–428. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
