

The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006
- PMID: 19249393
- PMCID: PMC2705939
- DOI: 10.1053/j.gastro.2008.12.047
The incidence, prevalence, and outcomes of patients with gastroparesis in Olmsted County, Minnesota, from 1996 to 2006
Abstract
Background & aims: The epidemiology of gastroparesis is unknown. We aimed to determine the incidence, prevalence, and outcome of gastroparesis in the community.
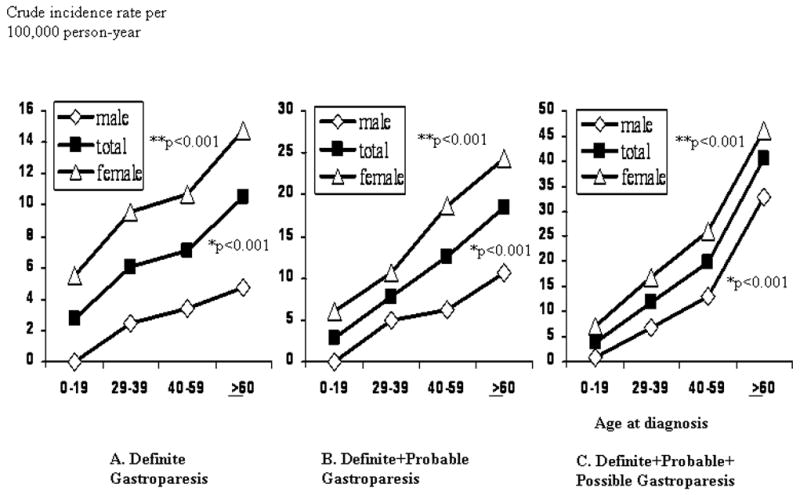
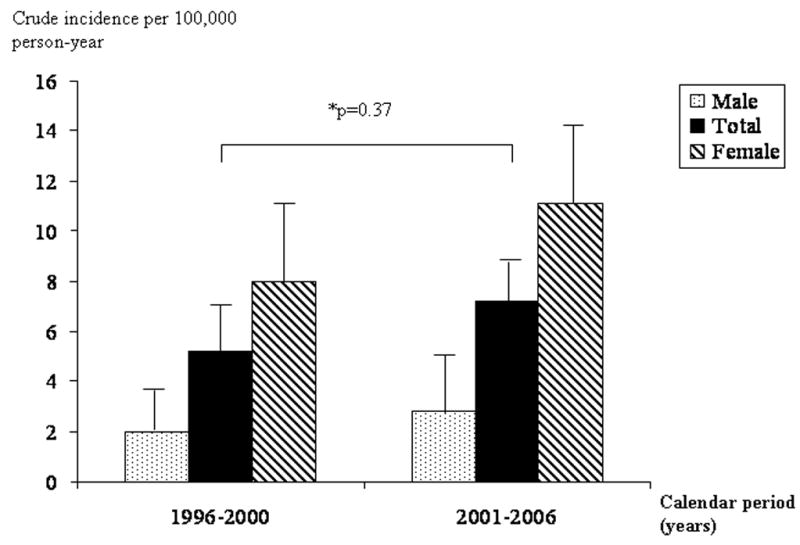
Methods: Using the Rochester Epidemiology Project, a medical records linkage system in Olmsted County, Minnesota, we identified county residents with potential gastroparesis. The complete medical records were reviewed by a gastroenterologist. Three diagnostic definitions were used: (1) definite gastroparesis, delayed gastric emptying by standard scintigraphy and typical symptoms for more than 3 months; (2) probable gastroparesis, typical symptoms and food retention on endoscopy or upper gastrointestinal study; (3) possible gastroparesis, typical symptoms alone or delayed gastric emptying by scintigraphy without gastrointestinal symptoms. Poisson regression was used to assess the association of incidence rates with age, sex, and calendar period.
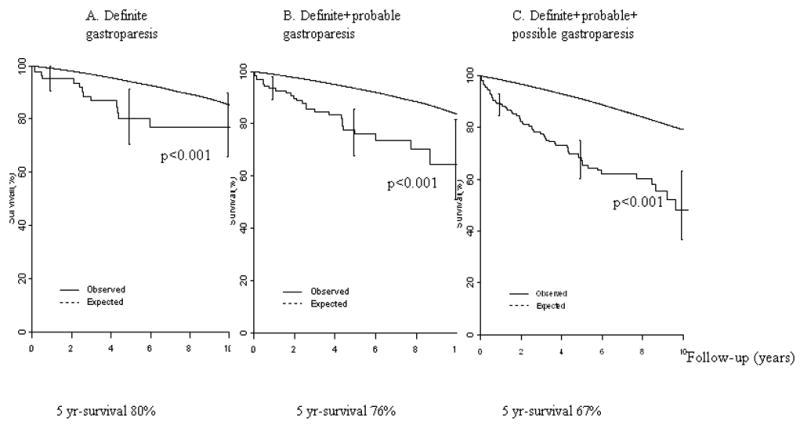
Results: Among 3604 potential cases of gastroparesis, 83 met diagnostic criteria for definite gastroparesis, 127 definite plus probable gastroparesis, and 222 any of the 3 definitions of gastroparesis. The age-adjusted (to the 2000 US white population) incidence per 100,000 person-years of definite gastroparesis for the years 1996-2006 was 2.4 (95% confidence interval [CI], 1.2-3.8) for men and 9.8 (95% CI, 7.5-12.1) for women. The age-adjusted prevalence of definite gastroparesis per 100,000 persons on January 1, 2007, was 9.6 (95% CI, 1.8-17.4) for men and 37.8 (95% CI, 23.3-52.4) for women. Overall survival was significantly lower than the age- and sex-specific expected survival computed from the Minnesota white population (P<.05).
Conclusions: Gastroparesis is an uncommon condition in the community but is associated with a poor outcome.
Figures
References
-
- Kassander P. Asymptomatic gastric retention in diabetics (gastroparesis diabeticorum) Ann Intern Med. 1958;48:797–812. - PubMed
-
- Revicki DA, Rentz AM, Dubois D, Kahrilas P, Stanghellini V, Talley NJ, Tack J. Development and validation of a patient-assessed gastroparesis symptom severity measure: the Gastroparesis Cardinal Symptom Index. Aliment Pharmacol Ther. 2003;18:141–50. - PubMed
-
- Soykan I, Sivri B, Sarosiek I, Kiernan B, McCallum RW. Demography, clinical characteristics, psychological and abuse profiles, treatment, and long-term follow-up of patients with gastroparesis. Dig Dis Sci. 1998;43:2398–404. - PubMed
-
- Wang YR, Fisher RS, Parkman HP. Gastroparesis-Related Hospitalizations in the United States: Trends, Characteristics, and Outcomes, 1995–2004. Am J Gastroenterol. 2007;103:313–322. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
