

Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study
- PMID: 19249635
- PMCID: PMC2764235
- DOI: 10.1016/S0140-6736(09)60443-8
Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study
Abstract
Background: Atrial fibrillation contributes to substantial increases in morbidity and mortality. We aimed to develop a risk score to predict individuals' absolute risk of developing the condition, and to provide a framework for researchers to assess new risk markers.
Methods: We assessed 4764 participants in the Framingham Heart Study from 8044 examinations (55% women, 45-95 years of age) undertaken between June, 1968, and September, 1987. Thereafter, participants were monitored for the first event of atrial fibrillation for a maximum of 10 years. Multivariable Cox regression identified clinical risk factors associated with development of atrial fibrillation in 10 years. Secondary analyses incorporated routine echocardiographic measurements (5152 participants, 7156 examinations) to reclassify the risk of atrial fibrillation and to assess whether these measurements improved risk prediction.
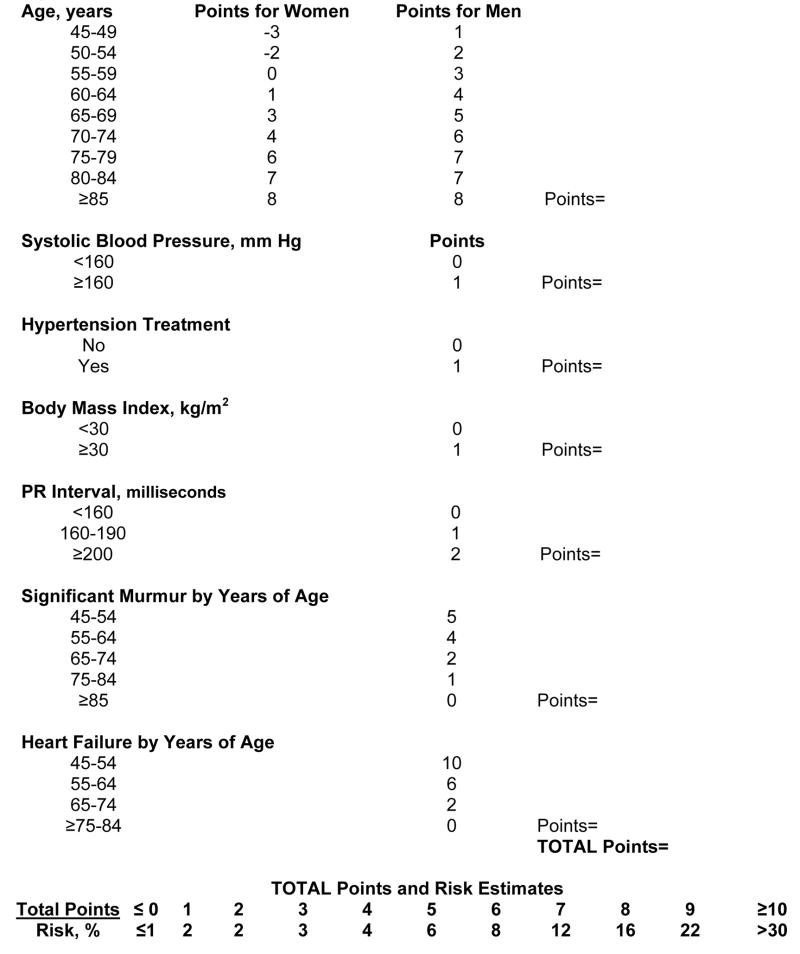
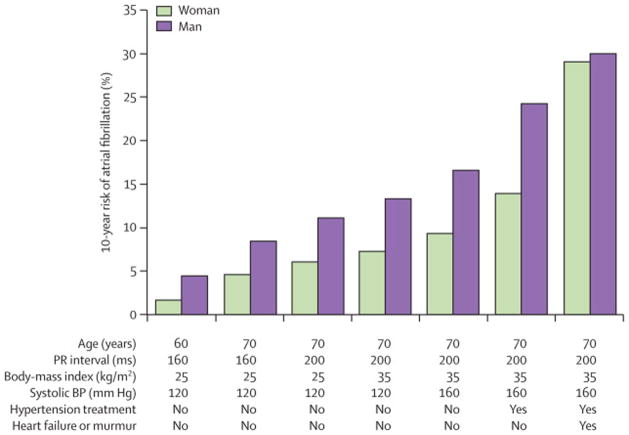
Findings: 457 (10%) of the 4764 participants developed atrial fibrillation. Age, sex, body-mass index, systolic blood pressure, treatment for hypertension, PR interval, clinically significant cardiac murmur, and heart failure were associated with atrial fibrillation and incorporated in a risk score (p<0.05, except body-mass index p=0.08), clinical model C statistic 0.78 (95% CI 0.76-0.80). Risk of atrial fibrillation in 10 years varied with age: more than 15% risk was recorded in 53 (1%) participants younger than 65 years, compared with 783 (27%) older than 65 years. Additional incorporation of echocardiographic measurements to enhance the risk prediction model only slightly improved the C statistic from 0.78 (95% CI 0.75-0.80) to 0.79 (0.77-0.82), p=0.005. Echocardiographic measurements did not improve risk reclassification (p=0.18).
Interpretation: From clinical factors readily accessible in primary care, our risk score could help to identify risk of atrial fibrillation for individuals in the community, assess technologies or markers for improvement of risk prediction, and target high-risk individuals for preventive measures.
Figures


Comment in
-
Delirium cordis: can we predict the onset of atrial fibrillation?Lancet. 2009 Feb 28;373(9665):698-700. doi: 10.1016/S0140-6736(09)60415-3. Lancet. 2009. PMID: 19249615 No abstract available.
-
Predicting atrial fibrillation.Lancet. 2009 May 2;373(9674):1523; author reply 1523-4. doi: 10.1016/S0140-6736(09)60857-6. Lancet. 2009. PMID: 19410714 No abstract available.
References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–5. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–25. - PubMed
-
- Benjamin EJ, Wolf PA, D’Agostino RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. - PubMed
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Seward JB, et al. Coronary ischemic events after first atrial fibrillation: risk and survival. Am J Med. 2007;120:357–63. - PubMed
-
- Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003;107:2920–5. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-25195/HC/NHLBI NIH HHS/United States
- R01 HL071039/HL/NHLBI NIH HHS/United States
- R01 HL104156/HL/NHLBI NIH HHS/United States
- N01 HC025195/HC/NHLBI NIH HHS/United States
- R01 HL077477/HL/NHLBI NIH HHS/United States
- R56 AG029451/AG/NIA NIH HHS/United States
- HL080124/HL/NHLBI NIH HHS/United States
- AG028321/AG/NIA NIH HHS/United States
- N01 HC025195/HL/NHLBI NIH HHS/United States
- R01 AG029451/AG/NIA NIH HHS/United States
- R01 HL067288/HL/NHLBI NIH HHS/United States
- HL076784/HL/NHLBI NIH HHS/United States
- R01 HL093328/HL/NHLBI NIH HHS/United States
- R01 HL080124/HL/NHLBI NIH HHS/United States
- R01 NS017950/NS/NINDS NIH HHS/United States
- R01 NS 17950/NS/NINDS NIH HHS/United States
- R01 HL092577/HL/NHLBI NIH HHS/United States
- R01 HL064753/HL/NHLBI NIH HHS/United States
- AG029451/AG/NIA NIH HHS/United States
- R01 HL076784/HL/NHLBI NIH HHS/United States
- K24 HL004334/HL/NHLBI NIH HHS/United States
- R01 HL077447/HL/NHLBI NIH HHS/United States
- HL093328/HL/NHLBI NIH HHS/United States
- L30 HL097675/HL/NHLBI NIH HHS/United States
- HL71039/HL/NHLBI NIH HHS/United States
- R01 AG028321/AG/NIA NIH HHS/United States
- L30 HL082455/HL/NHLBI NIH HHS/United States
- 2K24 HL04334/HL/NHLBI NIH HHS/United States
- HL092577/HL/NHLBI NIH HHS/United States
- K23 HL080025/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
