

Who is monitoring your infections: shouldn't you be?
- PMID: 19250007
- PMCID: PMC2963596
- DOI: 10.1089/sur.2008.056
Who is monitoring your infections: shouldn't you be?
Abstract
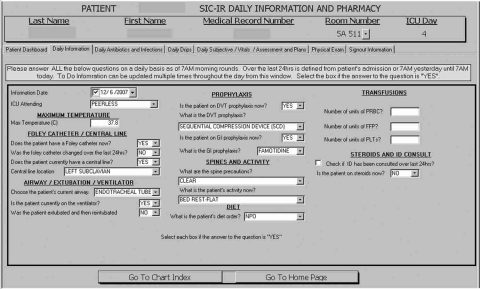
Background: In the era of pay for performance and outcome comparisons among institutions, it is imperative to have reliable and accurate surveillance methodology for monitoring infectious complications. The current monitoring standard often involves a combination of prospective and retrospective analysis by trained infection control (IC) teams. We have developed a medical informatics application, the Surgical Intensive Care-Infection Registry (SIC-IR), to assist with infection surveillance. The objectives of this study were to: (1) Evaluate for differences in data gathered between the current IC practices and SIC-IR; and (2) determine which method has the best sensitivity and specificity for identifying ventilator-associated pneumonia (VAP).
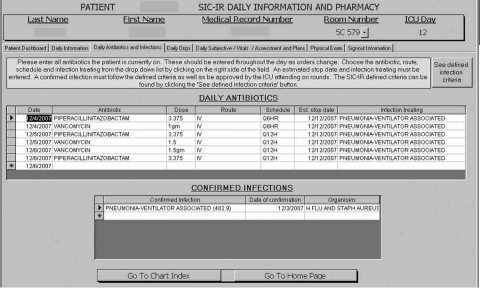
Methods: A prospective analysis was conducted in two surgical and trauma intensive care units (STICU) at a level I trauma center (Unit 1: 8 months, Unit 2: 4 months). Data were collected simultaneously by the SIC-IR system at the point of patient care and by IC utilizing multiple administrative and clinical modalities. Data collected by both systems included patient days, ventilator days, central line days, number of VAPs, and number of catheter-related blood steam infections (CR-BSIs). Both VAPs and CR-BSIs were classified using the definitions of the U.S. Centers for Disease Control and Prevention. The VAPs were analyzed individually, and true infections were defined by a physician panel blinded to methodology of surveillance. Using these true infections as a reference standard, sensitivity and specificity for both SIC-IR and IC were determined.
Results: A total of 769 patients were evaluated by both surveillance systems. There were statistical differences between the median number of patient days/month and ventilator-days/month when IC was compared with SIC-IR. There was no difference in the rates of CR-BSI/1,000 central line days per month. However, VAP rates were significantly different for the two surveillance methodologies (SIC-IR: 14.8/1,000 ventilator days, IC: 8.4/1,000 ventilator days; p = 0.008). The physician panel identified 40 patients (5%) who had 43 VAPs. The SIC-IR identified 39 and IC documented 22 of the 40 patients with VAP. The SIC-IR had a sensitivity and specificity of 97% and 100%, respectively, for identifying VAP and for IC, a sensitivity of 56% and a specificity of 99%.
Conclusions: Utilizing SIC-IR at the point of patient care by a multidisciplinary STICU team offers more accurate infection surveillance with high sensitivity and specificity. This monitoring can be accomplished without additional resources and engages the physicians treating the patient.
Figures
References
-
- Edwards JR. Peterson KD. Andrus ML, et al. National Healthcare Safety Network (NHSN) Report, data summary for 2006, issued June 2007. Am J Infect Control. 2007;35:290–301. - PubMed
-
- Pottinger JM. Herwaldt LA. Peri TM. Basics of surveillance: An overview. Infect Control Hosp Epidemiol. 1997;18:513–527. - PubMed
-
- Scheckler WE. Brimhall D. Buck AS, et al. Requirements for infrastructure and essential activities of infection control and epidemiology in hospitals: A consensus panel report. Society for Healthcare Epidemiology of America. Infect Control Hosp Epidemiol. 1998;19:114–124. - PubMed
-
- Delgado-Rodriguez M. Gomez-Ortega A. Sierra A, et al. The effect of frequency of chart review on the sensitivity of noso-comial infection surveillance in general surgery. Infect Control Hosp Epidemiol. 1999;20:208–212. - PubMed
-
- Belio-Blasco C. Torres-Fernandez-Gil MA. Echeverria-Echarri JL. Gomez-Lopez LI. Evaluation of two retrospective active surveillance methods for the detection of nosocomial infection in surgical patients. Infect Control Hosp Epidemiol. 2000;21:24–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
