

The burden of sepsis-associated mortality in the United States from 1999 to 2005: an analysis of multiple-cause-of-death data
- PMID: 19250547
- PMCID: PMC2688146
- DOI: 10.1186/cc7733
The burden of sepsis-associated mortality in the United States from 1999 to 2005: an analysis of multiple-cause-of-death data
Abstract
Introduction: Sepsis is the 10th leading cause of death in the United States. The National Center for Health Statistics' multiple-cause-of-death (MCOD) dataset is a large, publicly available, population-based source of information on disease burden in the United States. We have analysed MCOD data from 1999 to 2005 to investigate trends, assess disparities and provide population-based estimates of sepsis-associated mortality during this period.
Methods: Sepsis-associated deaths occurring in the United States from 1999 to 2005 were identified in MCOD data using International Classification of Disease, 10th Revision (ICD-10) codes. Population-based mortality rates were calculated using bridged-race population estimates from the National Center for Health Statistics. Comparisons across age, sex and racial/ethnic groups were achieved by calculating mortality rate ratios.
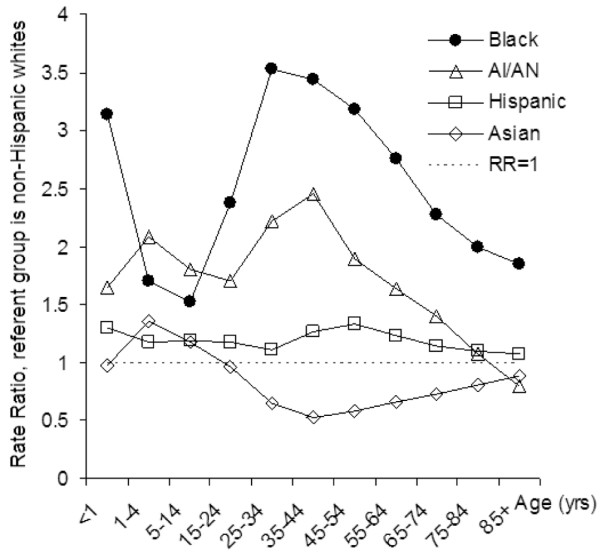
Results: From 1999 to 2005 there were 16,948,482 deaths in the United States. Of these, 1,017,616 were associated with sepsis (6.0% of all deaths). The age-adjusted rate of sepsis-associated mortality was 50.37 deaths per 100,000 (95% confidence interval (CI) = 50.28 to 50.47). There were significant disparities in sepsis-associated mortality in race/ethnicity and sex groups (P < 0.0001). After controlling for age, Asians were less likely than whites to experience sepsis-related death (rate ratio (RR) = 0.78, 95% CI = 0.77 to 0.78), while Blacks (RR = 2.24, 95% CI = 2.23 to 2.24), American Indians/Alaska Natives (RR = 1.24, 95% CI = 1.24 to 1.25) and Hispanics (RR = 1.14, 95% CI = 1.13 to 1.14) were more likely than whites to experience sepsis-related death. Men were at increased risk for sepsis-associated death in all race/ethnicity categories (RR = 1.27, 95% CI = 1.27 to 1.28), but the degree of increased susceptibility associated with being male differed among racial/ethnic groups (P < 0.0001). Although crude sepsis-associated mortality increased by 0.67% per year during the study period (P < 0.0001), the age-adjusted mortality rate decreased by 0.18% per year (P < 0.01).
Conclusions: The rapid rise in sepsis mortality seen in previous decades has slowed, but population ageing continues to drive the growth of sepsis-associated mortality in the United States. Disparities in sepsis-associated mortality mirror those previously reported for sepsis incidence. Sepsis in Asians, Hispanics and American Indian/Alaska Natives should be studied separately because aggregate measures may obscure important differences among these groups.
Figures
Comment in
-
'Relation, association, attribution ...' - the multiple faces of death in critical care medicine.Crit Care. 2009;13(2):138. doi: 10.1186/cc7789. Epub 2009 Apr 29. Crit Care. 2009. PMID: 19439049 Free PMC article.
References
-
- Kung HC, Hoert DL, Xu J, Murphy SL. National vital statistics reports. Vol. 56. No. 10. Hyattsville: National Center for Health Statistics; 2008. Deaths: final data for 2005. - PubMed
-
- Increase in National Hospital Discharge Survey rates for septicemia-United States, 1979–1987. MMWR Morb Mortal Wkly Rep. 1990;39:31–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
