

Practice patterns in screening for varices: an American survey
- PMID: 19251491
- PMCID: PMC3292195
- DOI: 10.1016/j.dld.2009.01.002
Practice patterns in screening for varices: an American survey
Abstract
Background and aims: Guidelines recommend screening for gastroesophageal varices. Regional studies suggest screening is underutilized, but information from across the United States is unavailable. We explored practice patterns and adherence to guidelines in a random sample of physicians and sought to define whether differences existed according to practice type, setting and years of practice.
Materials and methods: Surveys were randomly sent to 600 gastroenterologists and hepatologists. Descriptive data is presented as percentage and comparisons were performed by chi-square analysis. Significance was defined at a p value <0.05.
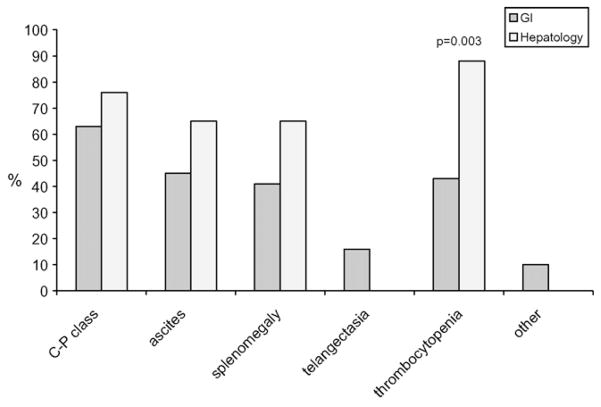
Results: 180 completed surveys were returned. Mean age was 48.9+/-10 years and 87% were male. 50% were community-based and 74% had been in practice >10 years. 53% (78% hepatologists versus 45% of gastroenterologists) screened consistently (>75% of the time), (p<0.001). No differences in screening frequency were found according to practice setting or years in practice. 62% screened all cirrhotics whereas 38% screened based on clinical characteristics. In patients without gastroesophageal varices, 60% repeated esophagogastroduodenoscopy in 2-3 years. In those with small gastroesophageal varices, repeat esophagogastroduodenoscopy was recommended in 1-2 years by 73%. In patients with small and large varices, 40% and 54% of physicians respectively, recommended prophylaxis. 6% of physicians recommend prophylaxis regardless of the presence or size of varices.
Conclusions: Screening for varices is under-implemented. Many screened based on clinical findings that have not been shown to reliably predict high-risk gastroesophageal varices. Continued education and removal of financial barriers to screening are central to increasing screening rates and improving patient outcomes.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Endoscopic treatment for gastroesophageal varices in patients with cirrhosis: a survey comparing between developed and developing countries.BMC Gastroenterol. 2025 Mar 15;25(1):176. doi: 10.1186/s12876-025-03758-6. BMC Gastroenterol. 2025. PMID: 40089662 Free PMC article.
-
Quality of Care Provided by Hepatologists to Patients with Cirrhosis at Three Parallel Health Systems.Dig Dis Sci. 2016 Oct;61(10):2857-2867. doi: 10.1007/s10620-016-4221-3. Epub 2016 Jun 11. Dig Dis Sci. 2016. PMID: 27289585
-
Facility- and Patient-Level Factors Associated with Esophageal Variceal Screening in the USA.Dig Dis Sci. 2016 Jan;61(1):62-9. doi: 10.1007/s10620-015-3865-8. Epub 2015 Sep 12. Dig Dis Sci. 2016. PMID: 26363933 Free PMC article.
-
Remaining challenges for the noninvasive diagnosis of esophageal varices in liver cirrhosis.Esophagus. 2020 Jan;17(1):19-24. doi: 10.1007/s10388-019-00699-4. Epub 2019 Oct 16. Esophagus. 2020. PMID: 31620917 Review.
-
Endoscopic screening for varices in cirrhosis: findings, implications, and outcomes.Gastroenterology. 2002 May;122(6):1620-30. doi: 10.1053/gast.2002.33419. Gastroenterology. 2002. PMID: 12016427 Review.
Cited by
-
Primary Prophylaxis for Variceal Bleeding and the Improved Survival of Patients with Newly Diagnosed Hepatocellular Carcinoma.Dig Dis Sci. 2016 Nov;61(11):3354-3362. doi: 10.1007/s10620-016-4255-6. Epub 2016 Jul 19. Dig Dis Sci. 2016. PMID: 27435325
-
Gastrointestinal endoscopy in cirrhotic patient: Issues on the table.World J Gastrointest Endosc. 2021 Jul 16;13(7):210-220. doi: 10.4253/wjge.v13.i7.210. World J Gastrointest Endosc. 2021. PMID: 34326942 Free PMC article. Review.
-
Overutilization of endoscopic surveillance in nondysplastic Barrett's esophagus: a multicenter study.Gastrointest Endosc. 2012 Jan;75(1):23-31.e2. doi: 10.1016/j.gie.2011.08.042. Epub 2011 Nov 17. Gastrointest Endosc. 2012. PMID: 22100301 Free PMC article.
References
-
- Smith JL, Graham DY. Variceal hemorrhage: a critical evaluation of survival analysis. Gastroenterology. 1982;82:968–73. - PubMed
-
- de Franchis R. Evolving consensus in portal hypertension. Report of the Baveno IV consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol. 2005;43:167–76. - PubMed
-
- Lowe RC, Grace ND. Primary prophylaxis of variceal hemorrhage. Clin Liver Dis. 2001;5:665–76. - PubMed
-
- D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment of portal hypertension: an evidence-based approach. Semin Liver Dis. 1999;19:475–505. - PubMed
-
- Merkel C, Marin R, Angeli P, Zanella P, Felder M, Bernardinello E, et al. A placebo-controlled clinical trial of nadolol in the prophylaxis of growth of small esophageal varices in cirrhosis. Gastroenterology. 2004;127:476–84. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
