

Patients' depression treatment preferences and initiation, adherence, and outcome: a randomized primary care study
- PMID: 19252046
- PMCID: PMC2710876
- DOI: 10.1176/ps.2009.60.3.337
Patients' depression treatment preferences and initiation, adherence, and outcome: a randomized primary care study
Abstract
Objective: The authors examined the association of treatment preferences with treatment initiation, adherence, and clinical outcome among nonsenior adult and senior primary care patients with depression.
Methods: Sixty primary care participants meeting DSM-IV criteria for major depression were randomly assigned to receive treatment congruent or incongruent with their primary stated preference. Participants received either 20 weeks of escitalopram, with monitoring by a care manager, or 12 weekly sessions of interpersonal psychotherapy followed by two monthly booster sessions. Adherence to treatment and depression severity were reassessed at weeks 4, 8, 12, and 24.
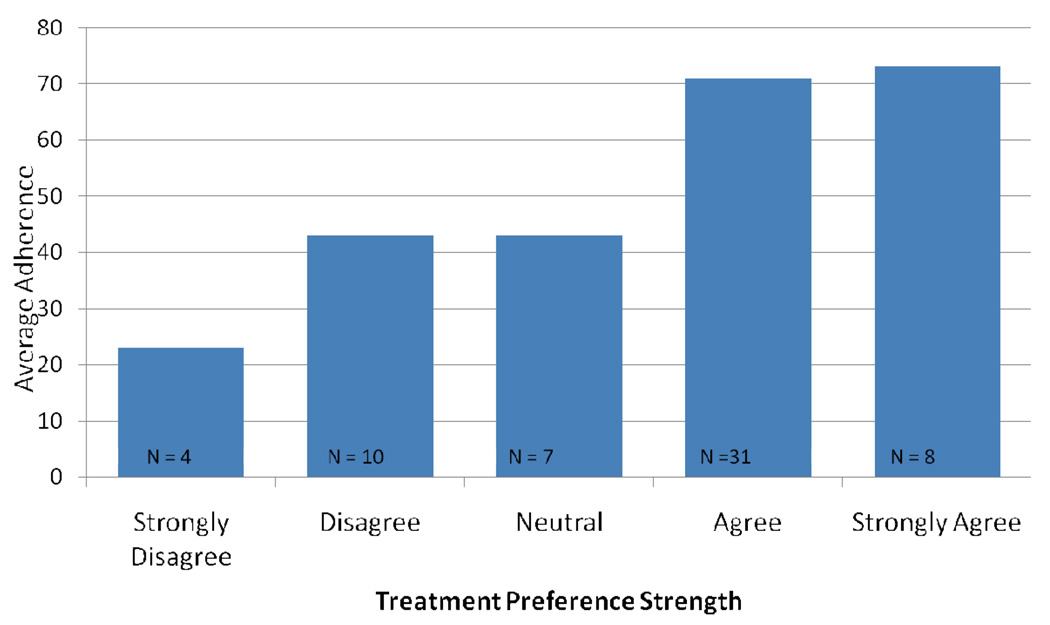
Results: Participants expressed stronger preferences for psychotherapy than for antidepressant medication. Preference strength was a more sensitive measure of outcome than was congruence versus incongruence of preference with the assigned treatment. Across age groups, preference strength was significantly associated with treatment initiation and 12-week adherence rate but not with depression severity or remission.
Conclusions: A continuous measure of preference strength may be a more useful measure in clinical practice than preferences per se. Future research should focus on whether and how greater facilitation of the treatment decision-making process between patient and clinician influences clinical outcome.
Figures



References
-
- Young AS, Klap R, Sherbourne CD, et al. The quality of care for depressive and anxiety disorders in the United States. Archives of General Psychiatry. 2001;58:55–61. - PubMed
-
- Klap R, Unroe KT, Unützer J. Caring for mental illness in the United States: a focus on older adults. American Journal of Geriatric Psychiatry. 2003;11:517–524. - PubMed
-
- Schulberg H, Block M, Madonia M, et al. Treating major depression in primary care practice. Eight-month clinical outcomes. Archives of General Psychiatry. 1996;53:913–919. - PubMed
-
- Cooper-Patrick L, Gonzales J, Rost K, et al. Patient preferences for treatment of depression. International Journal of Psychiatry in Medicine. 1998;28:382–383.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
