

Ventricular tachycardia and sudden cardiac death
- PMID: 19252119
- PMCID: PMC2664600
- DOI: 10.4065/84.3.289
Ventricular tachycardia and sudden cardiac death
Erratum in
- Mayo Clin Proc. 2009 May;84(5):483
Abstract
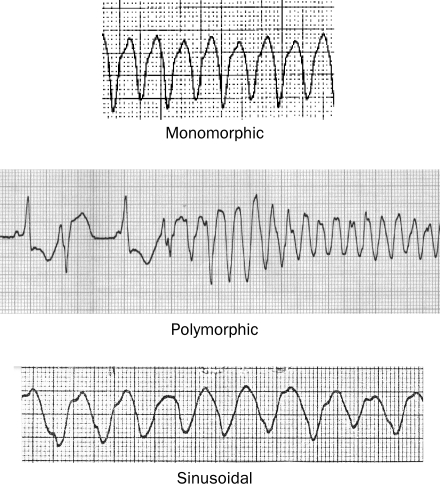
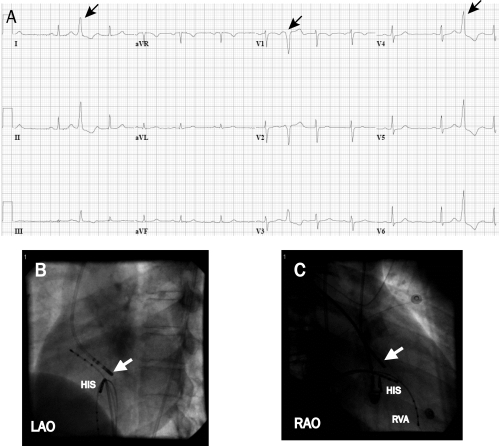
Ventricular tachycardia (VT), which most commonly occurs in patients with structural heart disease, can be associated with an increased risk of sudden death. The most common cause of ventricular fibrillation is acute coronary ischemia, whereas a myocardial scar from prior infarct is the most common cause of sustained monomorphic VT in patients with structural heart disease. More benign forms of idiopathic VT can also occur in the absence of structural heart disease. Treatment of VT involves both emergent management and prevention of recurrence with medical and device therapy. Appropriately selected patients who have experienced VT or those who are at risk of VT may be candidates for an implantable cardioverter-defibrillator. The left ventricular ejection fraction is most frequently used to stratify patients with either ischemic or nonischemic cardiomyopathy who are at risk of sudden death and may be candidates for a prophylactic defibrillator. Catheter ablation may also be an option for appropriately selected patients with many forms of VT. This article discusses the etiologies and management of VT and its association with sudden death.
Figures
References
-
- Coronel R, Fiolet JW, Wilms-Schopman JG, Opthof T, Schaapherder AF, Janse MJ. Distribution of extracellular potassium and electrophysiologic changes during two-stage coronary ligation in the isolated, perfused canine heart. Circulation 1989;80(1):165-177 - PubMed
-
- Pogwizd SM, Corr PB. Mechanisms underlying the development of ventricular fibrillation during early myocardial ischemia. Circ Res. 1990;66(3):672-695 - PubMed
-
- Wit AL, Allessie MA, Bonke FI, Lammers W, Smeets J, Fenoglio JJ., Jr Electrophysiologic mapping to determine the mechanism of experimental ventricular tachycardia initiated by premature impulses: experimental approach and initial results demonstrating reentrant excitation. Am J Cardiol. 1982;49(1):166-185 - PubMed
-
- El-Sherif N, Smith RA, Evans K. Canine ventricular arrhythmias in the late myocardial infarction period, 8: epicardial mapping of reentrant circuits. Circ Res. 1981;49(1):255-265 - PubMed
-
- Lloyd EA, Zipes DP, Heger JJ, Prystowsky EN. Sustained ventricular tachycardia due to bundle branch reentry. Am Heart J. 1982;104(5, pt 1):1095-1097 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
