

Urachal carcinoma: a clinicopathologic analysis of 24 cases with outcome correlation
- PMID: 19252435
- PMCID: PMC4225778
- DOI: 10.1097/PAS.0b013e31819aa4ae
Urachal carcinoma: a clinicopathologic analysis of 24 cases with outcome correlation
Abstract
Background: Urachal carcinomas occur mostly in the bladder dome, comprising 22% to 35% of vesical adenocarcinomas, and are generally treated by partial cystectomy with en bloc resection of the median umbilical ligament and umbilicus. Detailed pathologic studies with clinical outcome correlation are few.
Design: We reviewed histologic material and clinical data from 24 cases selected from a database of 67 dome-based tumors diagnosed and treated at our institution from 1984 to 2005. Follow-up information was available for all 24 patients.
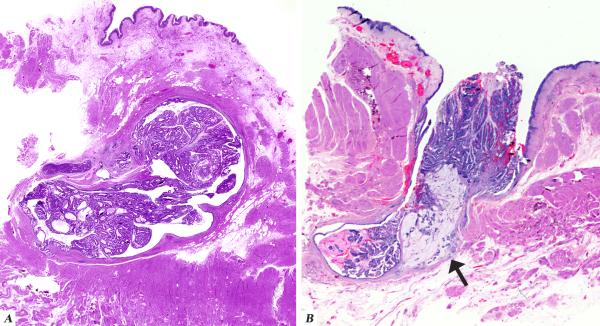
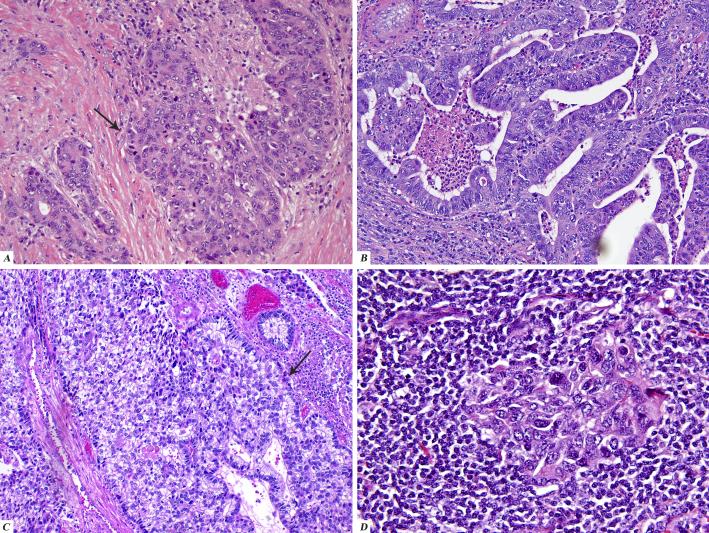
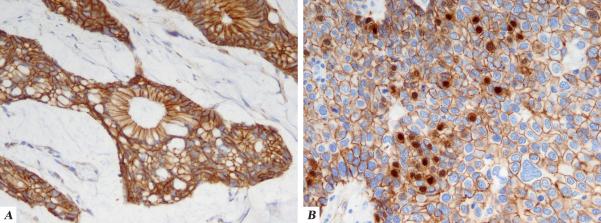
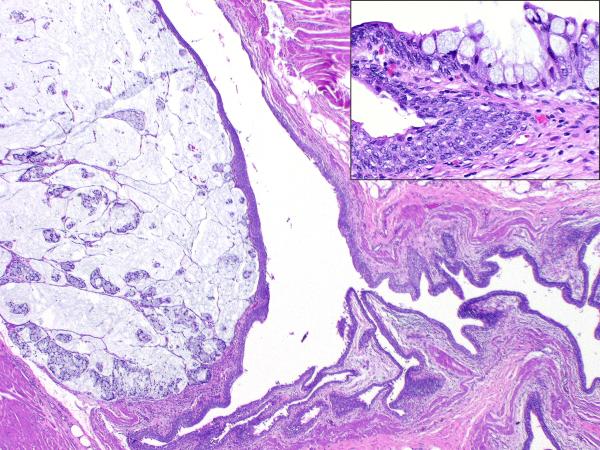
Result: The mean age at diagnosis was 52 years (range: 26 to 68 y). Fifteen patients were male and 9 were female. Location was the dome in 23 and dome and anterior wall in 1. Thirteen cases were pure adenocarcinoma, not otherwise specified, 9 were enteric type adenocarcinoma, and 2 were adenocarcinoma with focal components of lymphoepithelioma-like carcinoma and urothelial carcinoma with cytoplasmic clearing. Signet ring cell features were focally seen in 2 cases. Cystitis cystica and cystitis glandularis were seen in 4 and 2 cases, respectively. In all instances but 1, cystitis cystica/glandularis was focal and predominantly in the bladder overlying the urachal neoplasm. Urachal remnants were identified in 15 cases: the urachal epithelium was benign urothelial-type in 6 cases and showed adenomatous changes in 9. The overlying bladder urothelium was colonized by adenocarcinoma in 3 cases. In all 3, urachal remnants were identified and showed transition from benign to adenomatous epithelium. On immunohistochemistry, these tumors were positive for CK20 and variably positive for CK7 and 34BE12. The majority showed a cytoplasmic membranous staining pattern for beta-catenin, although in 1 case, focal nuclear immunoreactivity was identified. The Sheldon pathologic stage was pT1 in 0, pT2 in 2, pT3a in 8, pT3b in 11, pT3c in 1, pT4a in 1, and pT4b in 1 patient. One patient had a positive soft tissue margin. The mean follow-up period was 40 months (range: 0.3 to 157.6 mo). Seven of 24 (29%) cases recurred locally. The incidence of local recurrence was higher in patients who underwent a partial cystectomy alone (37.5%) versus those who had a more radical surgery (27%). Distant metastases occurred in 9 (37.5%) patients, 4 of whom had no prior local recurrence. Seven patients (29%) died of the disease. All cases with locally recurrent and metastatic disease belonged to stage pT3 or higher.
Conclusions: Pathologic stage is an important prognostic factor in urachal carcinoma. Surface urothelial involvement by carcinoma and presence of cystitis cystica/glandularis do not necessarily exclude the diagnosis of urachal carcinoma. Immunostains do not unequivocally discriminate a urachal from a colorectal carcinoma, but diffuse positivity for 34BE12 would support, and diffuse nuclear immunoreactivity for beta-catenin would militate against, a diagnosis of urachal carcinoma. Local recurrence may be owing to seeding within the distal urothelial tract, particularly in tumors with a configuration that is polypoid and which open into the bladder cavity. The type of surgery performed may have an effect on local recurrence despite negative margins of resection.
Figures
References
-
- Ashley RA, Inman BA, Sebo TJ, et al. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer. 2006;107:712–720. - PubMed
-
- Chu PG, Weiss LM. Keratin expression in human tissues and neoplasms. Histopathology. 2002;40:403–439. - PubMed
-
- Eble JN, Hull MT, Rowland RG, et al. Villous adenoma of the urachus with mucusuria: a light and electron microscopic study. J Urol. 1986;135:1240–1244. - PubMed
-
- Epstein JI, Amin MB, Reuter VE. Bladder biopsy interpretation. Lippincott Williams and Wilkins; Philadelphia:
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
