

Cytokine-producing dendritic cells in the pathogenesis of inflammatory skin diseases
- PMID: 19252974
- PMCID: PMC2874976
- DOI: 10.1007/s10875-009-9278-8
Cytokine-producing dendritic cells in the pathogenesis of inflammatory skin diseases
Abstract
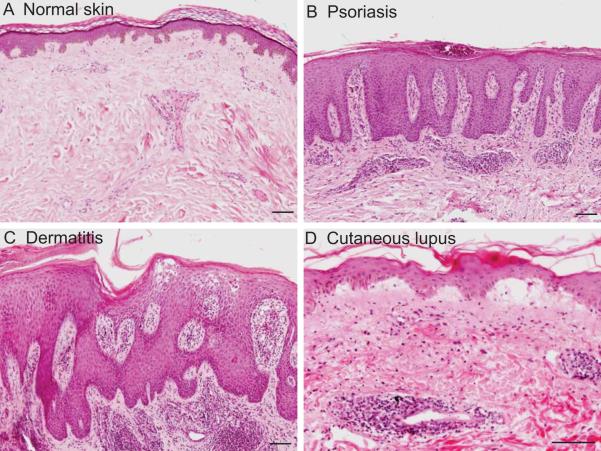
Introduction: Inflammatory skin diseases can be examined from many viewpoints. In this review, we consider three distinct cutaneous inflammatory diseases from the point of view of their major lesional dendritic cell (DC) subpopulations. The DC populations considered are Langerhans cells, myeloid DCs, and plasmacytoid DCs (pDCs), with specific attention to the presence and role of the inflammatory counterparts of these cells. From such a "dendritic cell-centric" focus, psoriasis, atopic dermatitis (AD), and cutaneous lupus erythematosus (CLE) are explored.
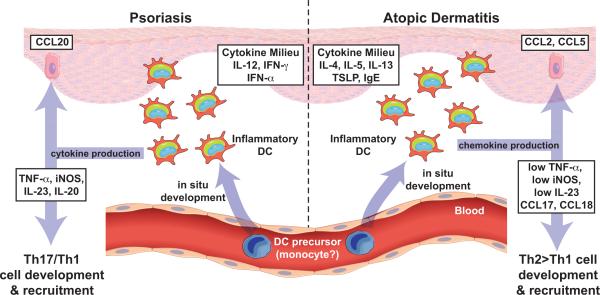
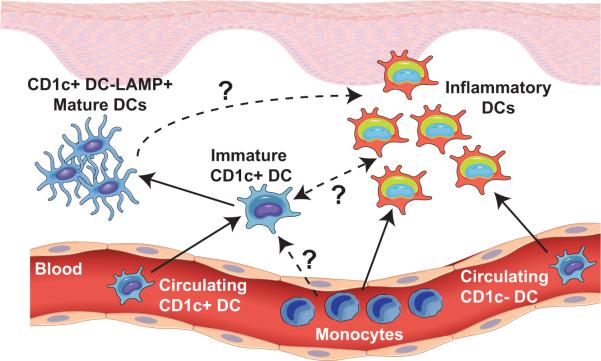
Discussion: In psoriasis, there is a specific population of myeloid "inflammatory" DCs that appears to play an important pathogenic role, while pDCs have been recently implicated in the initiation of psoriatic lesions. In AD, Langerhans cells may be important during initiation, while "inflammatory dendritic epidermal cells" (IDECs) appear to be abundant in lesional epidermis and dermis and contribute to maintenance of AD. These IDECs may actually be analogous to the myeloid inflammatory DCs found in the epidermal and dermal compartments of the skin in psoriasis, although they express distinct surface markers and induce different T cell polarities as a result of different cytokine milieu in which they develop. CLE has been recently characterized as a type I IFN-mediated disease, and pDCs are integral to the pathogenesis of this disease.
Conclusion: Thus, these DC subpopulations and their products will be reviewed in the context of these three cutaneous diseases to provide clinico-pathophysiological correlations between the lesional DCs, their products, and the skin diseases.
Figures
References
-
- Merad M, Ginhoux F, Collin M. Origin, homeostasis and function of Langerhans cells and other langerin-expressing dendritic cells. Nat Rev Immunol. 2008;8:935–47. - PubMed
-
- Ito T, Amakawa R, Inaba M, Hori T, Ota M, Nakamura K, Takebayashi M, Miyaji M, Yoshimura T, Inaba K, Fukuhara S. Plasmacytoid dendritic cells regulate Th cell responses through OX40 ligand and type I IFNs. J Immunol. 2004;172:4253–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
