

Phenotypic associations of Crohn's disease with antibodies to flagellins A4-Fla2 and Fla-X, ASCA, p-ANCA, PAB, and NOD2 mutations in a Swiss Cohort
- PMID: 19253375
- PMCID: PMC2732763
- DOI: 10.1002/ibd.20892
Phenotypic associations of Crohn's disease with antibodies to flagellins A4-Fla2 and Fla-X, ASCA, p-ANCA, PAB, and NOD2 mutations in a Swiss Cohort
Abstract
Background: Distinct Crohn's disease (CD) phenotypes correlate with antibody reactivity to microbial antigens. We examined the association between antibody response to 2 new flagellins called A4-Fla2 and Fla-X, anti-Saccharomyces cerevisiae antibodies (ASCA), anti-neutrophil cytoplasmic antibodies (p-ANCA), anti-pancreas antibodies (PAB), NOD2 mutations (R702W, G908R, and L1007fsinsC), and clinical CD phenotypes (according to Vienna criteria).
Methods: All the above-mentioned antibodies as well as NOD2 mutations were determined in 252 CD patients, 53 with ulcerative colitis (UC), and 43 healthy controls (HC) and correlated with clinical data.
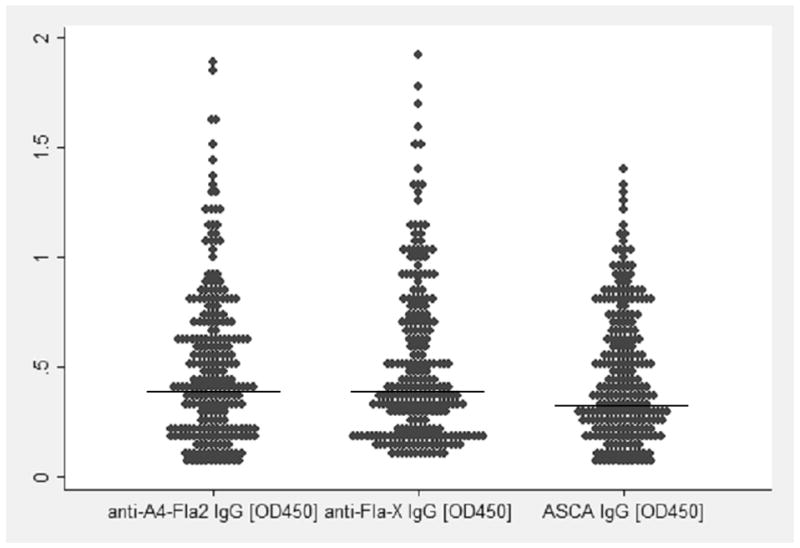
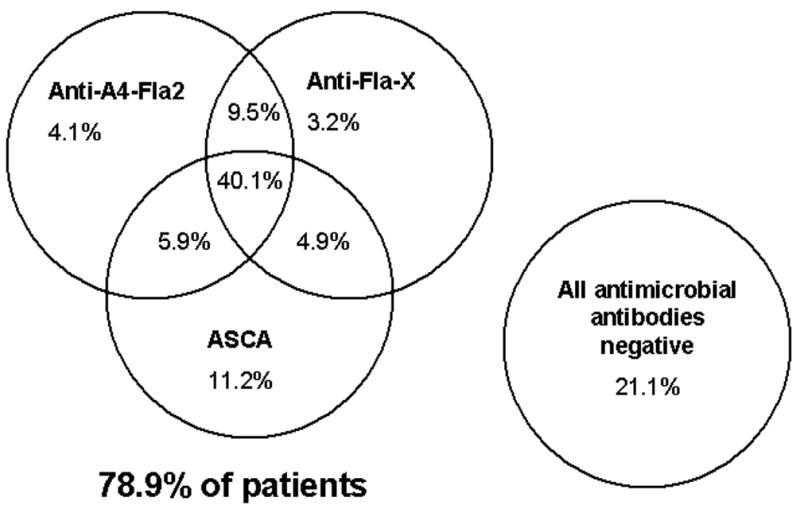
Results: A seroreactivity for A4-Fla2/Fla-X/ASCA/p-ANCA/PAB (in percent) was found in 59/57/62/12/22 of CD patients, 6/6/4/51/0 of UC patients, and 0/2/5/0/0 of healthy controls. CD behavior: 37% B1, 36% B2, and 27% B3. In multivariate logistic regression, antibodies to A4-Fla2, Fla-X, and ASCA were significantly associated with stricturing phenotype (P = 0.027, P = 0.041, P < 0.001), negative associations were found with inflammatory phenotype (P = 0.001, P = 0.005, P < 0.001). Antibodies to A4-Fla2, Fla-X, ASCA, and NOD2 mutations were significantly associated with small bowel disease (P = 0.013, P = 0.01, P < 0.001, P = 0.04), whereas ASCA was correlated with fistulizing disease (P = 0.007), and small bowel surgery (P = 0.009). Multiple antibody responses against microbial antigens were associated with stricturing (P < 0.001), fistulizing disease (P = 0.002), and small bowel surgery (P = 0.002).
Conclusions: Anti-flagellin antibodies and ASCA are strongly associated with complicated CD phenotypes. CD patients with serum reactivity against multiple microbes have the greatest frequency of strictures, perforations, and small bowel surgery. Further prospective longitudinal studies are needed to show that antibody-based risk stratification improves the clinical outcome of CD patients.
Conflict of interest statement
Conflict of interest: none
Figures
References
-
- Satsangi J, Morecroft J, Shah NB, et al. Genetics of inflammatory bowel disease: Scientific and clinical implications. Best Pract Res Clin Gastroenterol. 2003;17:3–18. - PubMed
-
- Bouma G, Strober W. The immunological and genetic basis of inflammatory bowel disease. Nat Rev Immunol. 2003;3:521–533. - PubMed
-
- D’Haens GR, Geboes K, Peeters M. Early lesions of recurrent Crohn’s disease caused by infusion of intestinal contents in excluded ileum. Gastroenterology. 1998;114:262–267. - PubMed
-
- Landers CJ, Cohavy O, Misra R, et al. Selected loss of tolerance evidenced by Crohn’s disease-associated immune responses to auto- and microbial antigens. Gastroenterology. 2002;123:689–699. - PubMed
-
- Adams RJ, Heazlewood SP, Gilshenan KS, et al. IgG antibodies against common gut bacteria are more diagnostic for Crohn’s disease than IgG against mannan or flagellin. Am J Gastroenterol. 2008;103:386–396. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical