

Diagnosing asthma in general practice with portable exhaled nitric oxide measurement--results of a prospective diagnostic study: FENO < or = 16 ppb better than FENO < or =12 ppb to rule out mild and moderate to severe asthma [added]
- PMID: 19254389
- PMCID: PMC2660901
- DOI: 10.1186/1465-9921-10-15
Diagnosing asthma in general practice with portable exhaled nitric oxide measurement--results of a prospective diagnostic study: FENO < or = 16 ppb better than FENO < or =12 ppb to rule out mild and moderate to severe asthma [added]
Erratum in
- Respir Res. 2009;10: 64 doi:10.1186/1465-9921-10-64
Abstract
Background: To evaluate the sensitivity, specificity and predictive values of fractional exhaled nitric oxide (FENO) for the diagnosis of asthma in general practice.
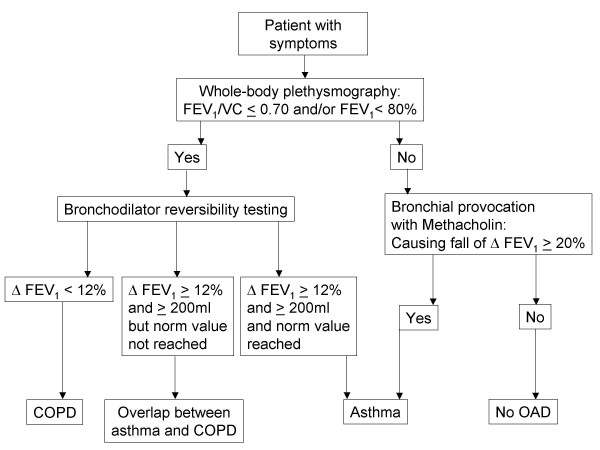
Methods: Prospective diagnostic study with 160 patients attending 10 general practices for the first time with complaints suspicious of obstructive airway disease (OAD). Patients were referred to a lung function laboratory for diagnostic investigation. The index test was FENO measured with a portable FENO analyser based on electrochemical sensor. The reference standard was the Tiffeneau ratio (FEV1/VC) as received by spirometric manoeuvre and/or results of bronchial provocation. Bronchial provocation with methacholine was performed to determine bronchial hyper-responsiveness (BHR) in the event of inconclusive spirometric results.
Results: 88 (55%) were female; their average age was 43.9 years. 75 (46.9%) patients had asthma, 25 (15.6%) had COPD, 8 (5.0%) had an overlap of COPD and asthma, and 52 (32.5%) had no OAD. At a cut-off level of 46 parts per billion (ppb) (n = 30; 18.8%), sensitivity was 32% (95%CI 23-43%), specificity 93% (95%CI 85-97%), positive predictive value (PPV) 80% (95%CI 63-91%), negative predictive value (NPV) 61% (95%CI 52-69%) when compared with a 20% fall in FEV1 from the baseline value (PC20) after inhaling methacholine concentration <or= 16 mg/ml. At 76 ppb (n = 11; 6.9%) specificity was 100% (95%CI 96-100%) and PPV was 100% (95%CI 72-100). At a cut-off level of 16 ppb (n = 68; 42.5%), sensitivity was 79% (95%CI 67-88), specificity 55% (95%CI 45-64), PPV 50% (95%CI 40-60), NPV 82% (95%CI 72-90 [corrected] when compared with a 20% fall of FEV1 after inhaling methacholine concentration <or= 4 mg/ml. Two [corrected] patients with unsuspicious spirometric results have to be tested with FENO to save one bronchial provocation test.
Conclusion: Asthma could be ruled in with FENO > 46 ppb. Mild and moderate to severe asthma could be ruled out with FENO <or= 16 ppb [corrected]. FENO measurement with an electrochemical sensor might be reasonable with respect to the time consuming procedure of bronchial provocation, which carries also some risk of severe bronchospasm. Further research is necessary to evaluate the effectiveness of this dual diagnostic strategy. The number needed to diagnose might be improved when the diagnostic precision could be enhanced by future technical developments.
Figures



References
-
- National Institute of Health Global Initiative for Asthma – Global Strategy for Asthma Management and Prevention (GINA) 2007. http://www.ginasthma.com
-
- Osborne ML, Pedula KL, O'Hollaren M, Ettinger KM, Stibolt T, Buist AS, Vollmer WM. Assessing future need for acute care in adult asthmatics: the Profile of Asthma Risk Study: a prospective health maintenance organization-based study. Chest. 2007;132:1151–1161. doi: 10.1378/chest.05-3084. - DOI - PubMed
-
- Kunzli N, Stutz EZ, Perruchoud AP, Brandli O, Tschopp JM, Bolognini G, Karrer W, Schindler C, Ackermann-Liebrich U, Leuenberger P. Peak flow variability in the SAPALDIA study and its validity in screening for asthma-related conditions. The SPALDIA Team. Am J Respir Crit Care Med. 1999;160:427–434. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
