

The prevalence and impact of anergia (lack of energy) in subjects with heart failure and its associations with actigraphy
- PMID: 19254674
- PMCID: PMC2705868
- DOI: 10.1016/j.cardfail.2008.10.021
The prevalence and impact of anergia (lack of energy) in subjects with heart failure and its associations with actigraphy
Abstract
Background: Anergia (lack of energy) is a newly delineated, criterion-based geriatric syndrome. Because heart failure (HF) is a common chronic condition among older adults and a because a cardinal symptom of HF is reduced energy, we characterized the degree of anergia in subjects with HF and evaluated its relevance to disease severity, functional performance, and quality of life.
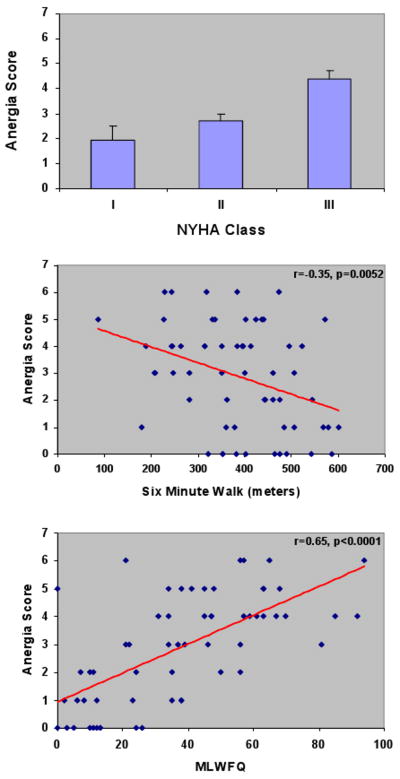
Methods and results: Prospective 3-month cohort study among a convenience sample of 61 subjects (61 +/- 15 years, 48% women, ejection fraction 41 +/- 16%) with New York Heart Association (NYHA) Class I-III HF were studied. The criterion for anergia was based on the major criterion "sits around for lack of energy" and any 2 of 6 minor criteria. Principal measures in addition to demographic and clinical characteristics included functional performance (NYHA class, 6-minute walk, cardiopulmonary exercise testing), plasma B-type natriuretic peptide, and quality of life (SF-12 and Minnesota Living with Heart Failure Questionnaire). To evaluate the relevance of anergia to daily function, each subject wore an Actigraph, a watch-like wrist device that continuously and automatically monitors patient activity levels and energy expenditure, for 3 months. Anergia was prevalent in 39% of this population. Anergia was associated with decrements in functional capacity (higher NYHA Class and lower 6-minute walk distance) as well as reduction in quality of life, but was not associated with ejection fraction. Actigraphy data demonstrated that HF subjects with anergia spent significantly less time performing moderate physical activity and the peak activity counts per day were significantly lower than HF subjects without anergia. Additionally, the amplitude of circadian rhythm was lower, suggesting altered sleep and activity patterns in HF subjects with anergia compared with those without anergia. Over the 3 months of follow-up, there was a significant association between anergia and intercurrent hospitalization.
Conclusions: Anergia is significantly associated with several of the cardinal domains of HF. Its presence is associated with demonstrable differences in both physical activity and circadian rhythm as measured by actigraphy and an increased risk of hospitalizations. Accordingly, anergia may be a target for intervention among HF subjects.
References
-
- Walke LM, Gallo WT, Tinetti ME, Fried TR. The burden of symptoms among community-dwelling older persons with advanced chronic disease. Arch Intern Med. 2004;164(21):2321–2324. - PubMed
-
- Heo S, Doering LV, Widener J, Moser DK. Predictors and effect of physical symptom status on health-related quality of life in patients with heart failure. Am J Crit Care. 2008;17(2):124–132. - PubMed
-
- Ekman I, Cleland JG, Swedberg K, Charlesworth A, Metra M, Poole-Wilson PA. Symptoms in patients with heart failure are prognostic predictors: insights from COMET. J Card Fail. 2005;11(4):288–292. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
