

Proximal humeral fracture as a risk factor for subsequent hip fractures
- PMID: 19255209
- PMCID: PMC2669747
- DOI: 10.2106/JBJS.G.01529
Proximal humeral fracture as a risk factor for subsequent hip fractures
Abstract
Background: With the aging of the world's population, the social and economic implications of osteoporotic fractures are at epidemic proportions. This study was performed to test the hypothesis that a proximal humeral fracture is an independent risk factor for a subsequent hip fracture and that the risk of the subsequent hip fracture is highest within the first five years after the humeral fracture.
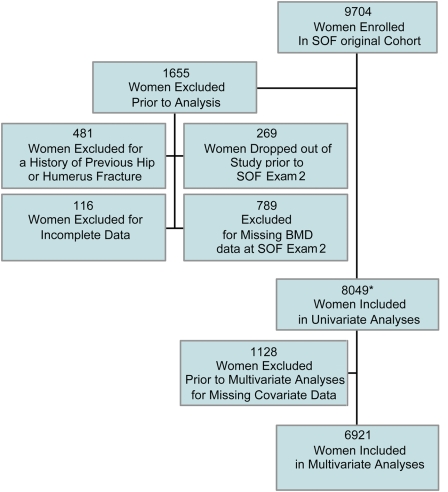
Methods: A cohort of 8049 older white women with no history of a hip or humeral fracture who were enrolled in the Study of Osteoporotic Fractures was followed for a mean of 9.8 years. The risk of hip fracture after an incident humeral fracture was estimated with use of age-adjusted Cox proportional hazards regression analysis with time-varying variables; women without a humeral fracture were the reference group. Cox regression analysis was used to evaluate the timing between the proximal humeral and subsequent hip fracture. Risk factors were determined on the basis of a review of the current literature, and we chose the variables that were most predictive and easily ascertained in a clinical setting.
Results: Three hundred and twenty-one women sustained a proximal humeral fracture, and forty-four of them sustained a subsequent hip fracture. After adjustment for age and bone mineral density, the hazard ratio for hip fracture for subjects with a proximal humeral fracture relative to those without a proximal humeral fracture was 1.83 (95% confidence interval = 1.32 to 2.53). After multivariate adjustment, this risk appeared attenuated but was still significant (hazard ratio = 1.57; 95% confidence interval = 1.12 to 2.19). The risk of a subsequent hip fracture after a proximal humeral fracture was highest within one year after the proximal humeral fracture, with a hazard ratio of 5.68 (95% confidence interval = 3.70 to 8.73). This association between humeral and hip fracture was not significant after the first year, with hazard ratios of 0.87 (95% confidence interval = 0.48 to 1.59) between one and five years after the humeral fracture and 0.58 (95% confidence interval = 0.22 to 1.56) after five years.
Conclusions: In this cohort of older white women, a proximal humeral fracture independently increased the risk of a subsequent hip fracture more than five times in the first year after the humeral fracture but was not associated with a significant increase in the hip fracture risk in subsequent years.
Figures
References
-
- Blackman DK, Kamimoto LA, Smith SM. Overview: surveillance for selected public health indicators affecting older adults—United States. MMWR CDC Surveill Summ. 1999;48:1-6. - PubMed
-
- Cummings SR, Rubin SM, Black D. The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen. Clin Orthop Relat Res. 1990;252:163-6. - PubMed
-
- Ray NF, Chan JK, Thamer M, Melton LJ 3rd. Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res. 1997;12:24-35. - PubMed
-
- Allander E, Gullberg B, Johnell O, Kanis JA, Ranstam J, Elffors L. Circumstances around the fall in a multinational hip fracture risk study: a diverse pattern for prevention. MEDOS Study Group. Mediterranean Osteoporosis Study. Accid Anal Prev. 1998;30:607-16. - PubMed
-
- Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality and costs. J Am Geriatr Soc. 2003;51:364-70. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
