

Pooled safety and efficacy analysis examining the effect of performance status on outcomes in nine first-line treatment trials using individual data from patients with metastatic colorectal cancer
- PMID: 19255311
- PMCID: PMC2669760
- DOI: 10.1200/JCO.2008.20.2879
Pooled safety and efficacy analysis examining the effect of performance status on outcomes in nine first-line treatment trials using individual data from patients with metastatic colorectal cancer
Erratum in
- J Clin Oncol. 2009 Jul 10;27(20):3410-1
Abstract
Purpose: Performance status (PS) is a prognostic factor in patients with metastatic colorectal cancer. Clinical trials typically enroll less than 10% of patients with a PS of 2 (PS2); thus, the benefit of systemic chemotherapy in PS2 patients is uncertain.
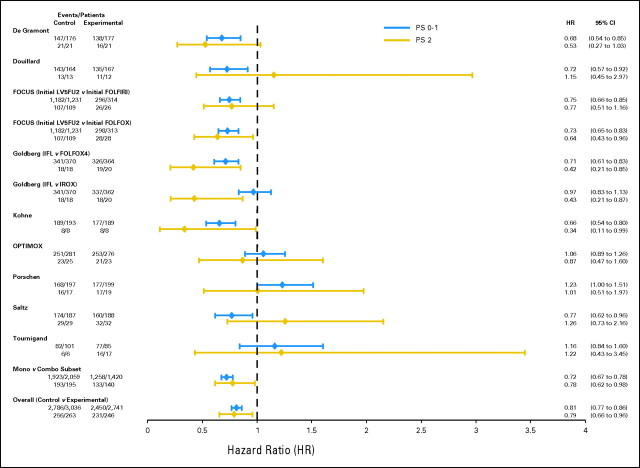
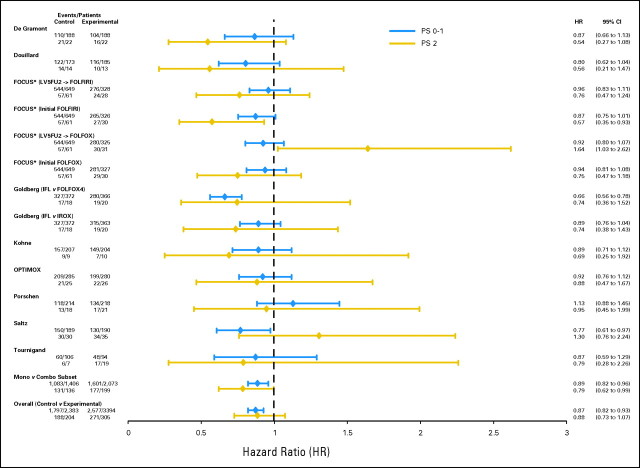
Patients and methods: Individual data from 6,286 patients (509 PS2 patients) from nine clinical trials were used to compare treatment efficacy by PS. Progression-free survival (PFS), grade > or = 3 adverse events, 60-day all-cause mortality, overall survival (OS), and response rate (RR) were explored in the full set of nine trials and in the five trials comparing first-line monotherapy with combination therapy.
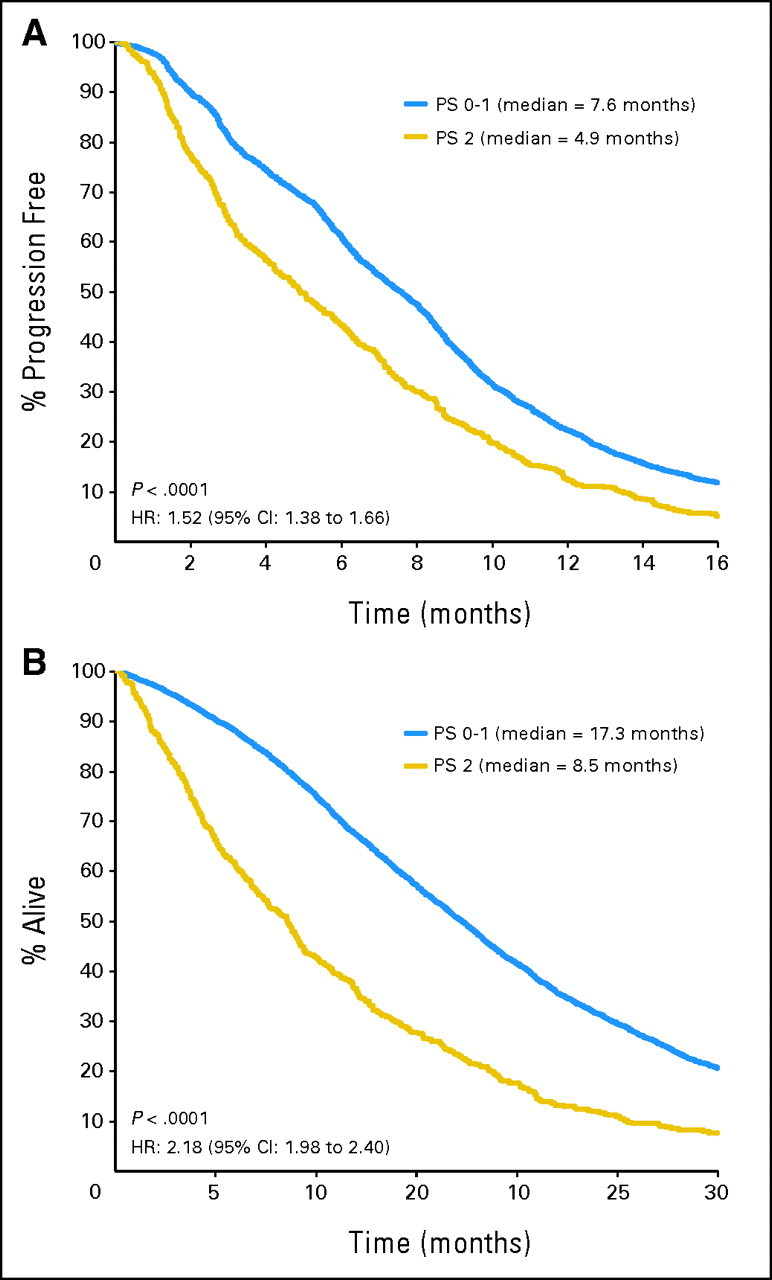
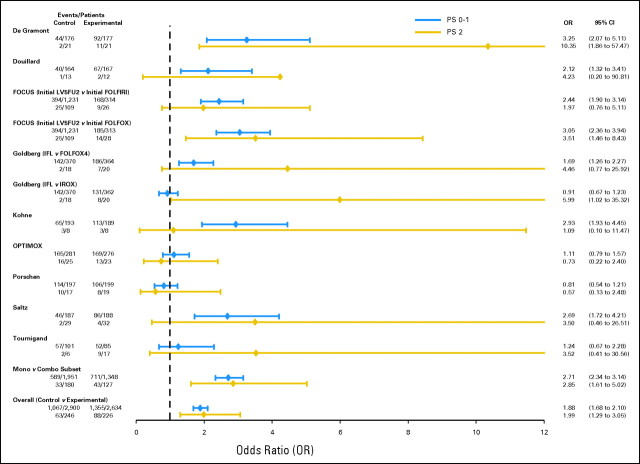
Results: Compared with patients with PS of 0 or 1, PS2 patients had significantly higher rates of grade > or = 3 nausea (8.5% v 16.4%, respectively; P < .0001) and vomiting (7.6% v 11.9%, respectively; P = .006) and 60-day all-cause mortality (2.8% v 12.0%, respectively; P < .0001). PS2 was prognostic for PFS (hazard ratio [HR] = 1.52; P < .0001; median PFS, 7.6 months for PS 0 or 1 v 4.9 months for PS2), OS (HR = 2.18; P < .0001; median OS, 17.3 months for PS 0 or 1 v 8.5 months for PS2), and RR (odds ratio = 0.61; P < .0001; 43.8% for PS 0 or 1 v 32.0% for PS2). The relative benefit and toxicity of experimental versus control treatment and monotherapy versus combination therapy were not different in PS 0 or 1 patients versus PS2 patients.
Conclusion: In clinical trials, PS2 patients derive similar benefit from superior treatment as patients with PS of 0 to 1 but with an increased risk of toxicities and 12% 60-day mortality. Although current treatment provides benefit, new approaches are required to approach 1-year median survival for PS2 patients.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Seymour MT, Maughan TS, Ledermann JA, et al. Different strategies of sequential and combination chemotherapy for patients with poor prognosis advanced colorectal cancer (MRC FOCUS): A randomised controlled trial. Lancet. 2007;370:143–152. - PubMed
-
- Koopman M, Antonini NF, Douma J, et al. Sequential versus combination chemotherapy with capecitabine, irinotecan, and oxaliplatin in advanced colorectal cancer (CAIRO): A phase III randomised controlled trial. Lancet. 2007;370:135–142. - PubMed
-
- de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000;18:2938–2947. - PubMed
-
- Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer: Irinotecan Study Group. N Engl J Med. 2000;343:905–914. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
