

Phase II trial of sorafenib in metastatic thyroid cancer
- PMID: 19255327
- PMCID: PMC2668972
- DOI: 10.1200/JCO.2008.18.2717
Phase II trial of sorafenib in metastatic thyroid cancer
Abstract
Purpose: Based on the pivotal role of Ras-Raf-MAP-ERK signaling and vascular endothelial growth factor (VEGF) in papillary thyroid cancer (PTC), we conducted a phase II clinical trial of sorafenib targeting RAF and VEGF receptor kinases in PTC.
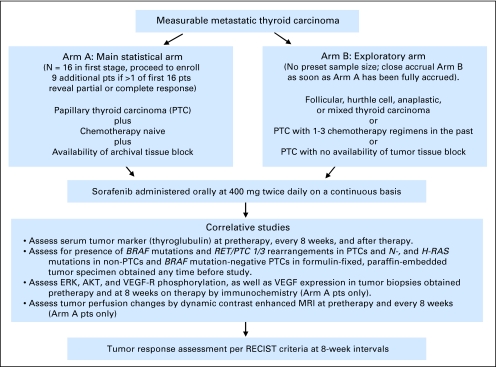
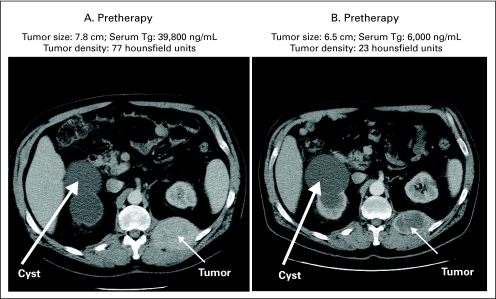
Patients and methods: The primary end point was the objective response rate. Secondary end points included response correlation with serum thyroglobulin (Tg); functional imaging; tumor genotype; and signaling inhibition in tumor biopsies. Using a Simon minimax two-stage design, 16 or 25 chemotherapy-naïve metastatic PTC patients were to be enrolled in arm A (accessible tumor for biopsy). Arm B patients had other subtypes of thyroid carcinoma or prior chemotherapy, and did not require tumor biopsies. Patients received 400 mg orally twice per day of sorafenib. Response was assessed every 2 months using RECIST (Response Evaluation Criteria in Solid Tumors).
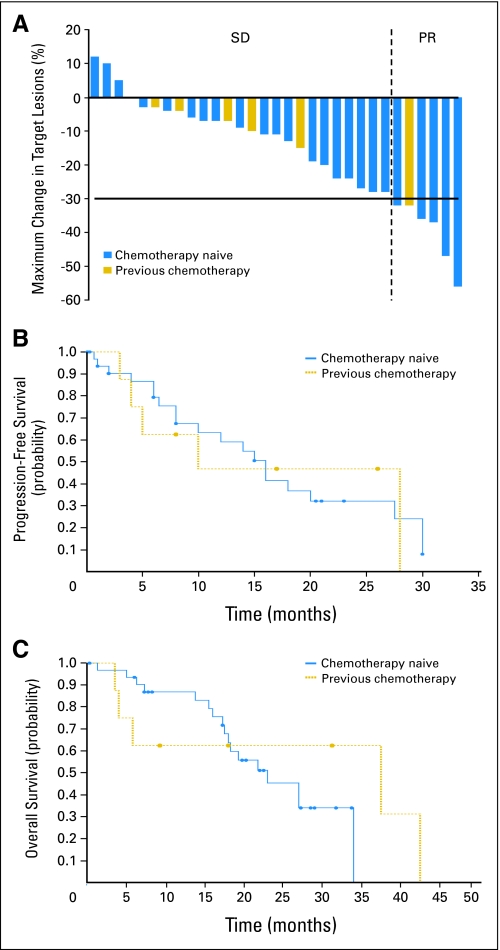
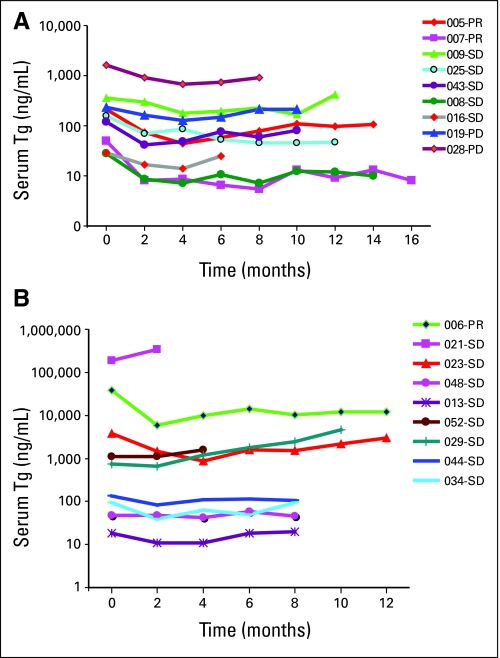
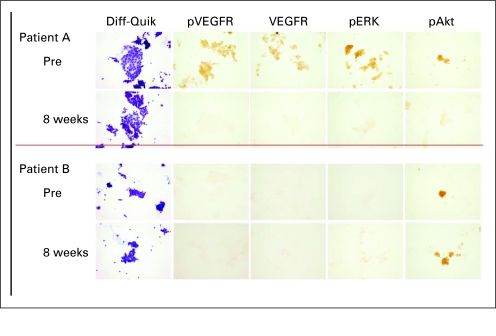
Results: Of 41 PTC patients, six patients had a partial response (PR; 15%; 95% CI, 6 to 29) and 23 patients (56%; 95% CI, 40 to 72) had stable disease longer than 6 months. Median duration of PR was 7.5 months (range, 6 to 14). Median progression-free survival was 15 months (95% CI, 10 to 27.5). In 14 (78%) of 18 Tg-assessable PTC patients, Tg declined more than 25%. Common grade 3 adverse events included hand-foot skin reaction, musculoskeletal pain, and fatigue. BRAF mutation was detected in 17 (77%) of 22 PTCs analyzed. Four of 10 paired tumor biopsies from PTC patients showed a reduction in levels of vascular endothelial growth factor receptor phosphorylation, ERK phosphorylation, and in VEGF expression during sorafenib therapy. No PRs were noted among non-PTC patients.
Conclusion: Sorafenib is reasonably well-tolerated therapy with clinical and biologic antitumor activity in metastatic PTC.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

References
-
- Cohen Y, Xing M, Mambo E, et al. BRAF mutation in papillary thyroid carcinoma. J Natl Cancer Inst. 2003;95:625–627. - PubMed
-
- Fukushima T, Suzuki S, Mashiko M, et al. BRAF mutations in papillary carcinomas of the thyroid. Oncogene. 2003;22:6455–6457. - PubMed
-
- Kimura ET, Nikiforova MN, Zhu Z, et al. High prevalence of BRAF mutations in thyroid cancer: Genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 2003;63:1454–1457. - PubMed
-
- Nikiforova MN, Kimura ET, Gandhi M, et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab. 2003;88:5399–5404. - PubMed
-
- Soares P, Trovisco V, Rocha AS, et al. BRAF mutations and RET/PTC rearrangements are alternative events in the etiopathogenesis of PTC. Oncogene. 2003;22:4578–4580. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
