

Common and distinct amygdala-function perturbations in depressed vs anxious adolescents
- PMID: 19255377
- PMCID: PMC2891508
- DOI: 10.1001/archgenpsychiatry.2008.545
Common and distinct amygdala-function perturbations in depressed vs anxious adolescents
Abstract
Context: Few studies directly compare amygdala function in depressive and anxiety disorders. Data from longitudinal research emphasize the need for such studies in adolescents.
Objective: To compare amygdala response to varying attention and emotion conditions among adolescents with major depressive disorder (MDD) or anxiety disorders, relative to adolescents with no psychopathology.
Design: Case-control study.
Setting: Government clinical research institute.
Participants: Eighty-seven adolescents matched on age, sex, intelligence, and social class: 26 with MDD (14 with and 12 without anxiety disorders), 16 with anxiety disorders but no depression, and 45 without psychopathology.
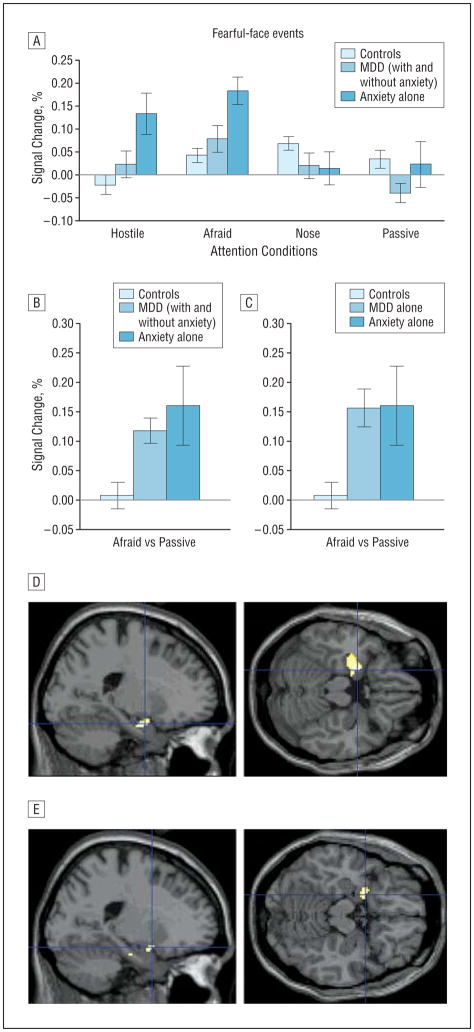
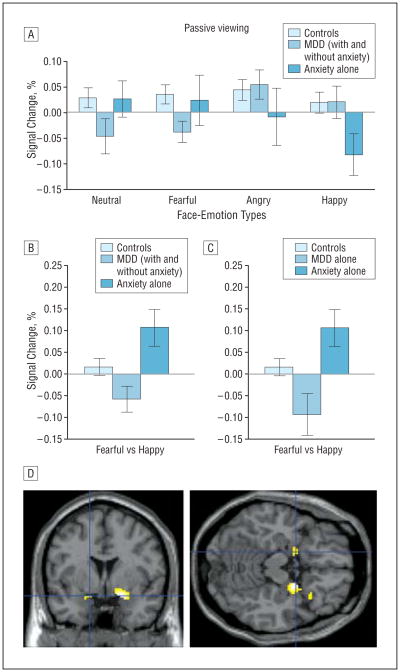
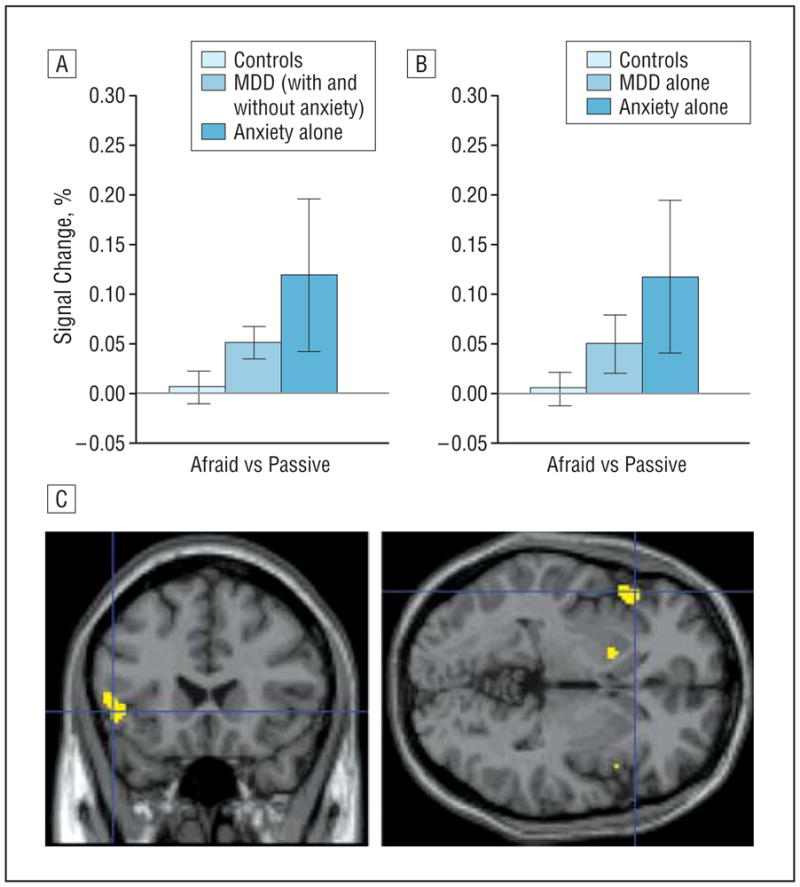
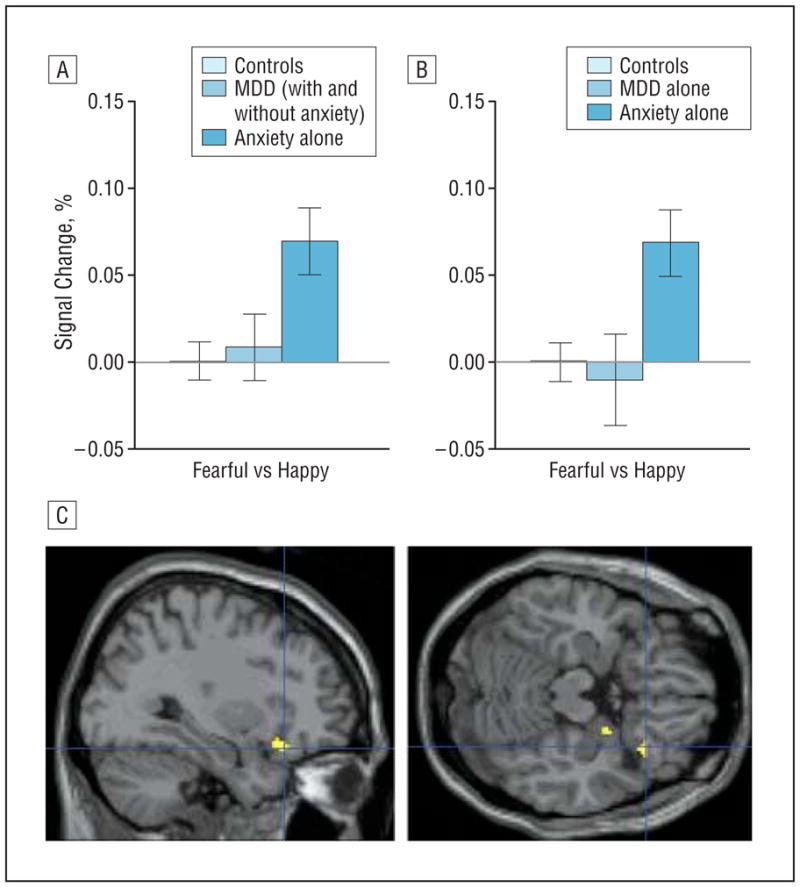
Main outcome measures: Blood oxygen level-dependent signal in the amygdala, measured by means of event-related functional magnetic resonance imaging. During imaging, participants viewed facial expressions (neutral, fearful, angry, and happy) while attention was constrained (afraid, hostility, and nose-width ratings) or unconstrained (passive viewing).
Results: Left and right amygdala activation differed as a function of diagnosis, facial expression, and attention condition both when patients with comorbid MDD and anxiety were included and when they were excluded (group x emotion x attention interactions, P < or = .03). Focusing on fearful face-viewing events, patients with anxiety and those with MDD both differed in amygdala responses from healthy participants and from each other during passive viewing. However, both MDD and anxiety groups, relative to healthy participants, exhibited similar signs of amygdala hyperactivation to fearful faces when subjectively experienced fear was rated.
Conclusions: Adolescent MDD and anxiety disorders exhibit common and distinct functional neural correlates during face processing. Attention modulates the degree to which common or distinct amygdala perturbations manifest in these patient groups, relative to healthy peers.
Figures
Similar articles
-
Amygdala function and 5-HTT gene variants in adolescent anxiety and major depressive disorder.Biol Psychiatry. 2009 Feb 15;65(4):349-55. doi: 10.1016/j.biopsych.2008.08.037. Epub 2008 Oct 31. Biol Psychiatry. 2009. PMID: 18950748 Free PMC article.
-
Association of Irritability and Anxiety With the Neural Mechanisms of Implicit Face Emotion Processing in Youths With Psychopathology.JAMA Psychiatry. 2017 Jan 1;74(1):95-103. doi: 10.1001/jamapsychiatry.2016.3282. JAMA Psychiatry. 2017. PMID: 27902832 Free PMC article.
-
Amygdala and nucleus accumbens activation to emotional facial expressions in children and adolescents at risk for major depression.Am J Psychiatry. 2008 Jan;165(1):90-8. doi: 10.1176/appi.ajp.2007.06111917. Epub 2007 Nov 6. Am J Psychiatry. 2008. PMID: 17986682
-
Rethinking the Use of Neutral Faces as a Baseline in fMRI Neuroimaging Studies of Axis-I Psychiatric Disorders.J Neuroimaging. 2017 May;27(3):281-291. doi: 10.1111/jon.12403. Epub 2016 Nov 2. J Neuroimaging. 2017. PMID: 27805291 Review.
-
Subgenual anterior cingulate cortex and hippocampal volumes in depressed youth: The role of comorbidity and age.J Affect Disord. 2016 Jan 15;190:726-732. doi: 10.1016/j.jad.2015.10.064. Epub 2015 Nov 12. J Affect Disord. 2016. PMID: 26600415 Review.
Cited by
-
Neuroimaging studies of pediatric social anxiety: paradigms, pitfalls and a new direction for investigating the neural mechanisms.Biol Mood Anxiety Disord. 2013 Jul 12;3:14. doi: 10.1186/2045-5380-3-14. eCollection 2013. Biol Mood Anxiety Disord. 2013. PMID: 23849682 Free PMC article. Review.
-
Emotion-Related Network Reorganization Following Fish Oil Supplementation in Depressed Bipolar Offspring: An fMRI Graph-Based Connectome Analysis.J Affect Disord. 2021 Sep 1;292:319-327. doi: 10.1016/j.jad.2021.05.086. Epub 2021 Jun 5. J Affect Disord. 2021. PMID: 34139404 Free PMC article. Clinical Trial.
-
An Exploratory Study on Resting-State Functional Connectivity in Individuals with Disorganized Attachment: Evidence for Key Regions in Amygdala and Hippocampus.Brain Sci. 2021 Nov 19;11(11):1539. doi: 10.3390/brainsci11111539. Brain Sci. 2021. PMID: 34827538 Free PMC article.
-
Adolescents' depressive symptoms moderate neural responses to their mothers' positive behavior.Soc Cogn Affect Neurosci. 2012 Jan;7(1):23-34. doi: 10.1093/scan/nsr049. Epub 2011 Sep 14. Soc Cogn Affect Neurosci. 2012. PMID: 21917846 Free PMC article.
-
Grant Report on Anxiety-CBT: Dimensional Brain Behavior Predictors of CBT Outcomes in Pediatric Anxiety.J Psychiatr Brain Sci. 2020;5:e200005. doi: 10.20900/jpbs.20200005. Epub 2020 Feb 28. J Psychiatr Brain Sci. 2020. PMID: 32258423 Free PMC article.
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication [published correction appears in Arch Gen Psychiatry. 2005;62(7):768] Arch Gen Psychiatry. 2005;62(6):593–602. - PubMed
-
- Wittchen H-U, Lieb R, Schuster P, Oldehinkel AJ. When is onset? investigations into early developmental stages of anxiety and depressive disorders. In: Rapoport JL, editor. Childhood Onset of “Adult” Psychopathology, Clinical and Research Advances. Washington, DC: American Psychiatric Press; 1999. pp. 259–302.
-
- Lieb R, Isensee B, Höfler M, Pfister H, Wittchen H-U. Parental major depression and the risk of depressive and other mental disorders in offspring: a prospective-longitudinal community study. Arch Gen Psychiatry. 2002;59(4):365–374. - PubMed
-
- Weissman MM, Wickramaratne P, Nomura Y, Warner V, Pilowsky D, Verdeli H. Offspring of depressed parents: 20 years later. Am J Psychiatry. 2006;163 (6):1001–1008. - PubMed
-
- Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. 1998;55(1):56–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
