

Should we test for CYP2C9 before initiating anticoagulant therapy in patients with atrial fibrillation?
- PMID: 19255811
- PMCID: PMC2669861
- DOI: 10.1007/s11606-009-0927-7
Should we test for CYP2C9 before initiating anticoagulant therapy in patients with atrial fibrillation?
Abstract
Background: Genetic variants of the warfarin sensitivity gene CYP2C9 have been associated with increased bleeding risk during warfarin initiation. Studies also suggest that such patients remain at risk throughout treatment.
Objective: Would testing patients with non-valvular atrial fibrillation (AF) for CYP2C9 before initiating warfarin improve outcomes?
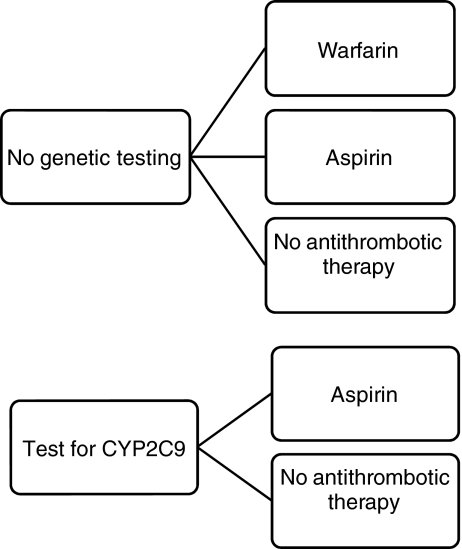
Design: Markov state transition decision model.
Setting: Ambulatory or inpatient settings necessitating new initiation of anticoagulation.
Patients: The base case was a 69-year-old man with newly diagnosed non-valvular AF. Interventions included: (1) warfarin, (2) aspirin, or (3) no antithrombotic therapy without genetic testing; and genetic testing followed by (4) aspirin or (5) no antithrombotic therapy in those with culprit CYP2C9 alleles.
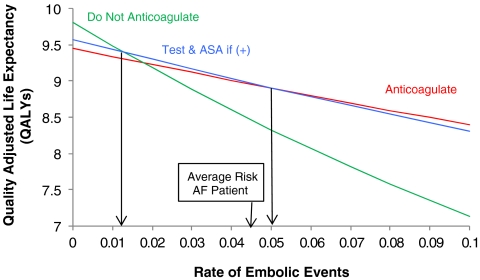
Measures: Quality-adjusted life years (QALYs).
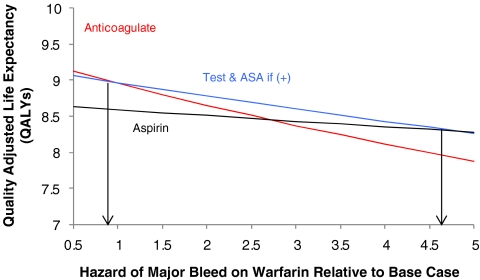
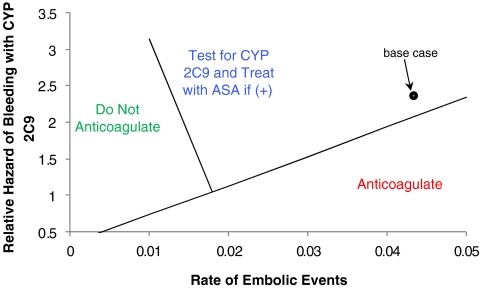
Results: In the base case, testing and treating patients with CYP2C9*2 and/or CYP2C9*3 with aspirin rather than warfarin was best (8.97 QALYs). However, warfarin without genetic testing was a close second (8.96 QALYs), a difference of roughly 5 days. Sensitivity analyses demonstrated that genetic testing followed by aspirin was best for patients at lower risk of embolic events. Warfarin without testing was preferred if the rate of embolic events was greater than 5% per year, or the risk of major bleeding while receiving warfarin was lower.
Conclusion: For patients at average risk for ischemic stroke due to AF and at average risk for major hemorrhage, treatment based on genetic testing offers no benefit compared to warfarin initiation without testing. The gain from testing may be larger in patients at lower risk of embolic events or at greater risk of bleeding.
Figures
Comment in
-
Testing for CYP2C9 before initiating anticoagulant therapy.J Gen Intern Med. 2009 Aug;24(8):992; author reply 993. doi: 10.1007/s11606-009-1041-6. J Gen Intern Med. 2009. PMID: 19506969 Free PMC article. No abstract available.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1161/CIRCULATIONAHA.106.177292', 'is_inner': False, 'url': 'https://doi.org/10.1161/circulationaha.106.177292'}, {'type': 'PubMed', 'value': '16908781', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16908781/'}]}
- Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006; 14(7):e257–354. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1378/chest.126.3_suppl.429S', 'is_inner': False, 'url': 'https://doi.org/10.1378/chest.126.3_suppl.429s'}, {'type': 'PubMed', 'value': '15383480', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15383480/'}]}
- Singer DE, Albers GW, Dalen JE, Go AS, Halperin JL, Manning WJ. Antithrombotic therapy in atrial fibrillation: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 suppl):429S–456S. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.jacc.2003.11.028', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.jacc.2003.11.028'}, {'type': 'PubMed', 'value': '15028346', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15028346/'}]}
- Rockson SG, Albers GW. Comparing the guidelines: anticoagulation therapy to optimize stroke prevention in patients with atrial fibrillation. J Am Coll Cardiol. 2004;43(6):929–35. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1002/ajmg.a.30391', 'is_inner': False, 'url': 'https://doi.org/10.1002/ajmg.a.30391'}, {'type': 'PubMed', 'value': '15714076', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15714076/'}]}
- Sanderson S, Emery J, Higgins J. CYP2C9 gene variants, drug dose, and bleeding risk in warfarin-treated patients: a HuGEnet systematic review and meta-analysis. Genet Med. 2005;7(2):97–104. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.thromres.2006.10.021', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.thromres.2006.10.021'}, {'type': 'PubMed', 'value': '17161452', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17161452/'}]}
- Yin T, Miyata T. Warfarin dose and the pharmacogenomics of CYP2C9 and VKORC1 - rationale and perspectives. Thromb Res. 2007;120(1):1–10. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
