

Patient-physician connectedness and quality of primary care
- PMID: 19258560
- PMCID: PMC2975389
- DOI: 10.7326/0003-4819-150-5-200903030-00008
Patient-physician connectedness and quality of primary care
Abstract
Background: Valid measurement of physician performance requires accurate identification of patients for whom a physician is responsible. Among all patients seen by a physician, some will be more strongly connected to their physician than others, but the effect of connectedness on measures of physician performance is not known.
Objective: To determine whether patient-physician connectedness affects measures of clinical performance.
Design: Population-based cohort study.
Setting: Academic network of 4 community health centers and 9 hospital-affiliated primary care practices.
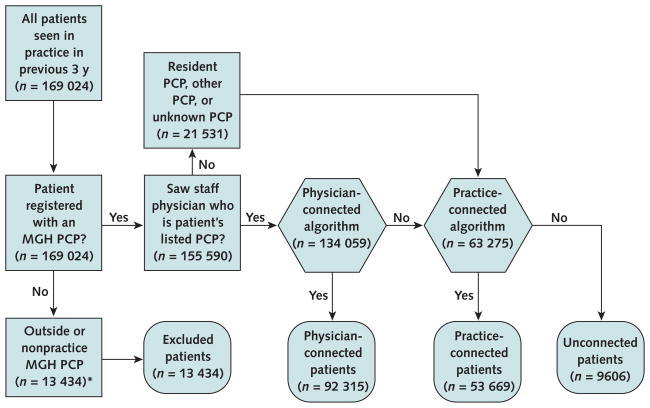
Patients: 155 590 adults with 1 or more visits to a study practice from 2003 to 2005.
Measurements: A validated algorithm was used to connect patients to either 1 of 181 physicians or 1 of 13 practices in which they received most of their care. Performance measures included breast, cervical, and colorectal cancer screening in eligible patients; hemoglobin A(1c) measurement and control in patients with diabetes; and low-density lipoprotein cholesterol measurement and control in patients with diabetes and coronary artery disease.
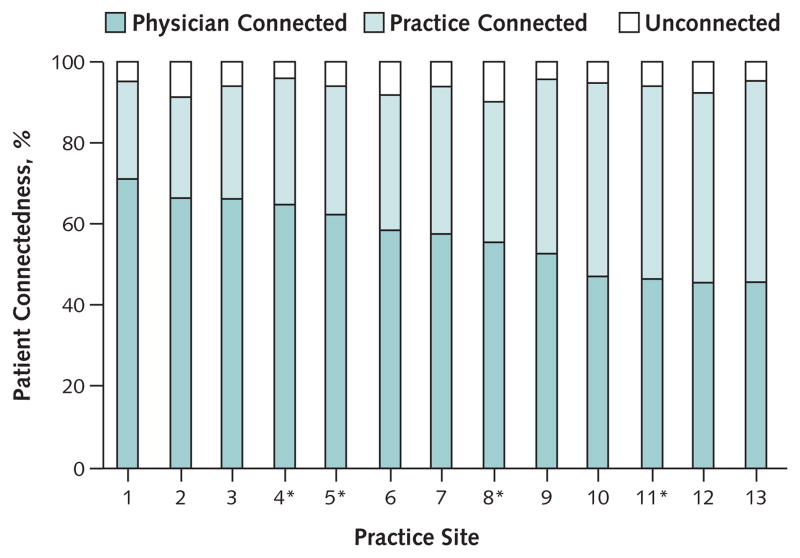
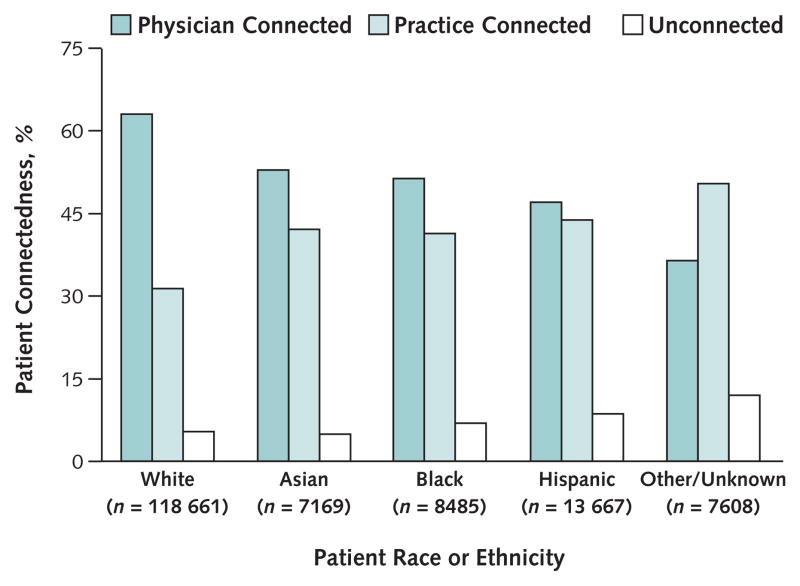
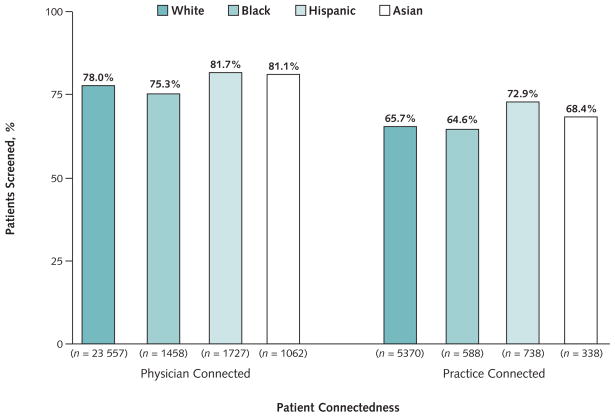
Results: Overall, 92 315 patients (59.3%) were connected to a specific physician, whereas 53 669 patients (34.5%) were connected only to a specific practice and 9606 patients (6.2%) could not be connected to a physician or practice. The proportion of patients in a practice who could be connected to a physician varied markedly (45.6% to 71.2% of patients per practice; P < 0.001). Physician-connected patients were significantly more likely than practice-connected patients to receive guideline-consistent care (for example, adjusted mammography rates were 78.1% vs. 65.9% [P < 0.001] and adjusted hemoglobin A(1c) rates were 90.3% vs. 74.9% [P < 0.001]). Receipt of preventive care varied more by whether patients were more or less connected to a physician than by race or ethnicity.
Limitation: Patient-physician connectedness was assessed in 1 primary care network.
Conclusion: Patients seen in primary care practices seem to be variably connected with a specific physician, and less connected patients are less likely to receive guideline-consistent care.
Funding: National Cancer Institute.
Conflict of interest statement
Figures
Comment in
-
Is there a personal doctor in the house?Ann Intern Med. 2009 Mar 3;150(5):351-2. doi: 10.7326/0003-4819-150-5-200903030-00012. Ann Intern Med. 2009. PMID: 19258561 No abstract available.
Summary for patients in
-
Summaries for patients. Patient-doctor connectedness and the quality of primary care.Ann Intern Med. 2009 Mar 3;150(5):I48. Ann Intern Med. 2009. PMID: 19258555 No abstract available.
References
-
- Ma J, Stafford RS. Quality of US outpatient care: temporal changes and racial/ethnic disparities. Arch Intern Med. 2005;165:1354–61. - PubMed
-
- Chassin MR, Galvin RW. The urgent need to improve health care quality. Institute of Medicine National Roundtable on Health Care Quality. JAMA. 1998;280:1000–5. - PubMed
-
- McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–45. - PubMed
-
- Starfield B. Primary Care: Concept, Evaluation, and Policy. New York: Oxford Univ Pr; 1992.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical