

Biology and treatment of metastatic gastrointestinal neuroendocrine tumors
- PMID: 19259290
- PMCID: PMC2633071
Biology and treatment of metastatic gastrointestinal neuroendocrine tumors
Abstract
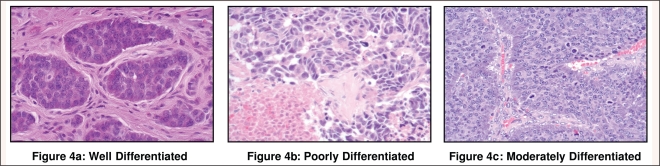
Neuroendocrine malignancies of the gastroenteropancreatic axis include carcinoid and pancreatic endocrine tumors. These heterogeneous neoplasms arise from the enterochromaffin cells of the gastrointestinal tract and the islet cells of the pancreas. Histologically, most well-differentiated endocrine tumors consist of small, round, monomorphic cells, arranged in islands or trabeculae, with a distinct "salt-and-pepper" pattern of nuclear chromatin. Chromogranin and synaptophysin are useful as immunohistochemical markers of neuroendocrine differentiation. Other common features include the capacity to secrete peptide hormones and biogenic amines. A relatively indolent growth rate is characteristic of most gastrointestinal neuroendocrine tumors, with the exception of poorly differentiated tumors which are usually aggressive. Treatment strategies are designed to limit tumor progression and palliate hormonal syndromes. This article reviews the diverse biologic characteristics of gastrointestinal neuroendocrine tumors and current treatment options for metastatic disease.
Figures
References
-
- Lubarsch O. Ueber den primären Krebs des Ileum, nebst Bemerkungen über das gleichzeitige Vorkommen von Krebs und Tuber - kolose. Virchows Arch. 1888;111:280–317.
-
- Oberndorfer S. Karzinoide Tumoren des Dünndarms. Frankf Z Pathol. 1907;1:425–429.
-
- Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97:934–959. - PubMed
-
- Thorson A, Biorck G, Bjorkman G, Walden-strom J. Malignant carcinoid of the small intestine with metastases to the liver, valvular disease of the right side of the heart (pulmonary stenosis and tricuspid regurgitation without septal defects), peripheral vasomotor symptoms, bronchoconstriction, and an unusual type of cyanosis; a clinical and pathologic syndrome. Am Heart J. 1954;47:795–817. - PubMed
LinkOut - more resources
Full Text Sources