

Aldosterone antagonists for preventing the progression of chronic kidney disease: a systematic review and meta-analysis
- PMID: 19261819
- PMCID: PMC2653663
- DOI: 10.2215/CJN.04750908
Aldosterone antagonists for preventing the progression of chronic kidney disease: a systematic review and meta-analysis
Abstract
Background and objectives: Addition of aldosterone antagonists (AA) might provide renal benefits to proteinuric chronic kidney disease (CKD) patients over and above the inhibition of renin-angiotensin system blockers (RAS). We evaluated the benefits and harms of adding selective and nonselective AA in CKD patients already on RAS.
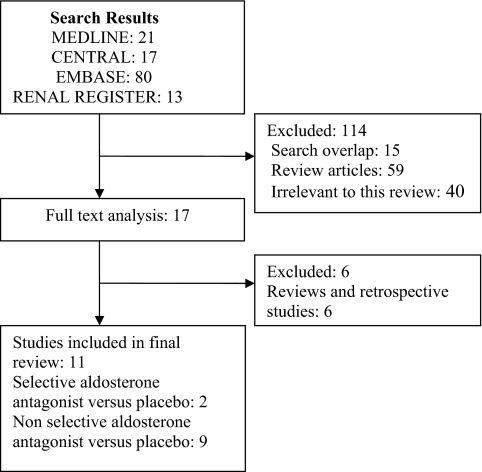
Design, setting, participants, & measurements: MEDLINE, EMBASE, and Renal Health Library were searched for relevant randomized clinical trials in adult CKD patients. Results were summarized using the random-effects model.
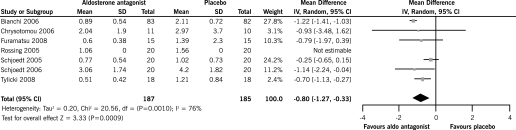
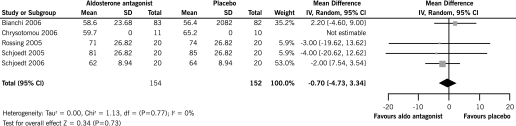
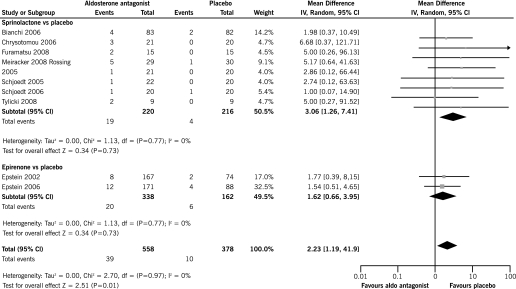
Results: Eleven trials (991 patients) were included. In comparison to angiotensin- converting enzyme inhibitors (ACEi) and/or angiotensin receptor blockers (ARB) plus placebo, nonselective AA along with ACEi and/or ARB significantly reduced 24 h proteinuria (seven trials, 372 patients, weighted mean difference [WMD] -0.80 g, 95% CI -1.27, -0.33) and BP. This did not translate into an improvement in GFR (WMD -0.70 ml/min/1.73m(2), 95% CI -4.73, 3.34). There was a significant increase in the risk of hyperkalemia with the addition of nonselective AA to ACEi and/or ARB (relative risk 3.06, 95% CI 1.26, 7.41). In two trials, addition of selective AA to ACEi resulted in an additional reduction in 24 h proteinuria, without any impact on BP and renal function. Data on cardiovascular outcomes, long-term renal outcomes and mortality were not available in any of the trials.
Conclusions: Aldosterone antagonists reduce proteinuria in CKD patients already on ACEis and ARBs but increase the risk of hyperkalemia. Long-term effects of these agents on renal outcomes, mortality, and safety need to be established.
Figures
Comment in
-
[What effect do aldosterone antagonists have in preventing chronic kidney disease progression?].Nefrologia. 2009;29(6 Suppl):43-5. doi: 10.3265/NEFROLOGIA.2009.29.S.E.noID.36.free. Nefrologia. 2009. PMID: 20221225 Spanish. No abstract available.
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Grassmann A, Gioberge S, Moeller S, Brown G: ESRD patients in 2004: Global overview of patient numbers, treatment modalities and associated trends. Nephrol Dial Transplant 20: 2587–2593, 2005 - PubMed
-
- Brenner B: Retarding the progression of renal disease. Kidney Int 64: 370–378, 2003 - PubMed
-
- Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, Striker G: The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. Modification of Diet in Renal Disease Study Group. N Engl J Med 330: 877–884, 1994 - PubMed
-
- Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S; RENAAL Study Investigators: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
