

New paradigm in the management of liver-only metastases from colorectal cancer
- PMID: 19262699
- PMCID: PMC2632517
New paradigm in the management of liver-only metastases from colorectal cancer
Abstract
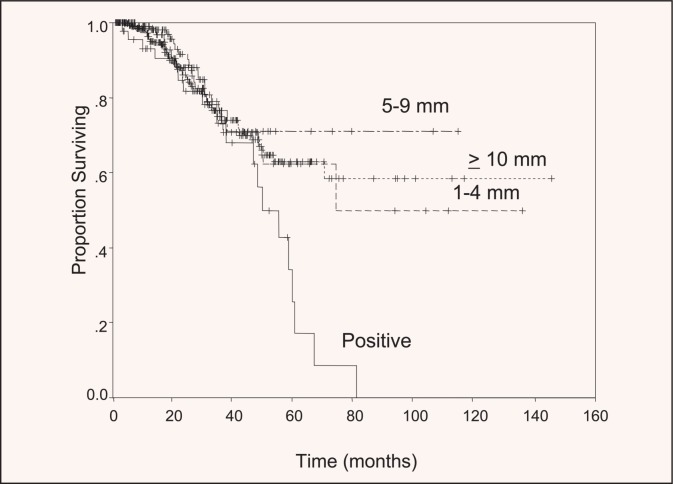
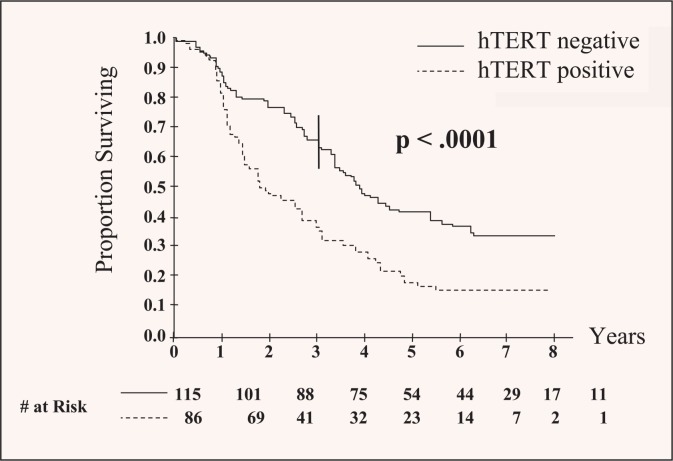
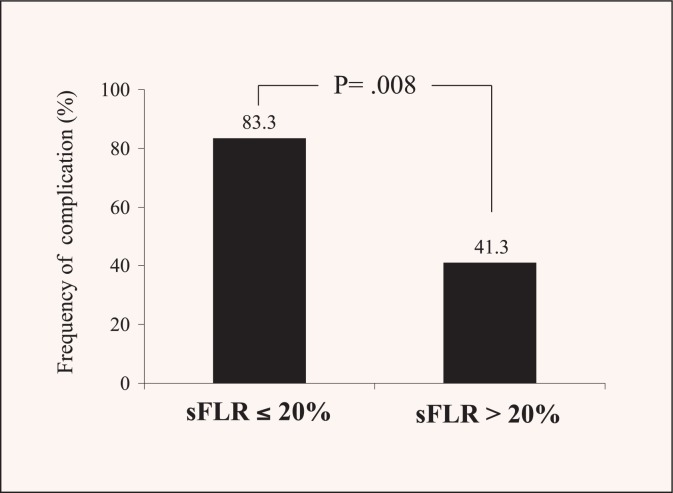
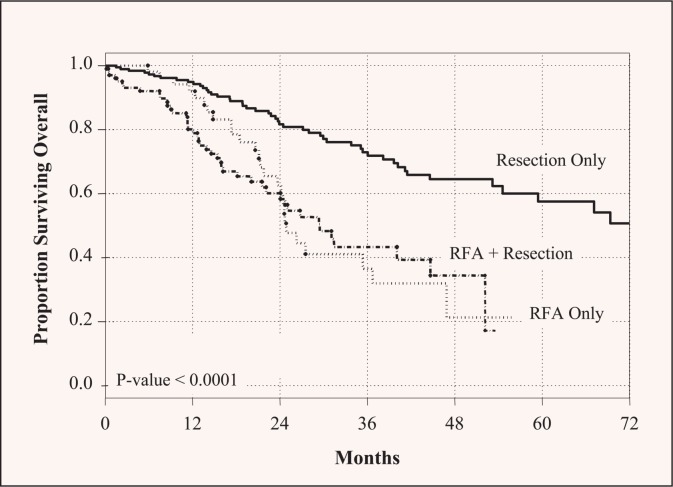
For patients with colorectal liver metastases, hepatic resection is the treatment of choice, and the 5-year survival rate following surgery now exceeds 50%. Timely multidisciplinary and multimodality approaches that may include preoperative systemic chemotherapy, preoperative portal vein embolization, extended hepatic resection, and two-stage hepatectomy, have enabled a large proportion of patients to undergo potentially curative treatment. The definition of resectability has shifted from a focus on tumor characteristics, such as tumor number and size, to determination of whether both intrahepatic and extrahepatic disease can be completely resected and whether such an approach is appropriate from an oncologic standpoint for a given patient. Future identification of molecular factors may aid in predicting prognosis of patients with colorectal liver metastases and in improving the selection of patients most likely to benefit from surgery. Hepatobiliary surgeons and medical oncologists should work together to individualize treatment strategies to maximize long-term survival in patients with colorectal liver metastases.
Figures
References
-
- Jemal A, Tiwari RC, Murray T, et al. Cancer statistics. CA Cancer J Clin. 2004;54:8–29. - PubMed
-
- Scheele J, Stangl R, Altendorf-Hofmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg. 1990;77:1241–1246. - PubMed
-
- Venook A. Critical evaluation of current treatments in metastatic colorectal cancer. Oncologist. 2005;10:250–261. - PubMed
-
- Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–2342. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources