

Re-evaluating the efficacy of beta-adrenergic agonists and antagonists in long QT-3 syndrome through computational modelling
- PMID: 19264765
- PMCID: PMC2682617
- DOI: 10.1093/cvr/cvp083
Re-evaluating the efficacy of beta-adrenergic agonists and antagonists in long QT-3 syndrome through computational modelling
Abstract
Aims: Long QT syndrome (LQTS) is a heterogeneous collection of inherited cardiac ion channelopathies characterized by a prolonged electrocardiogram QT interval and increased risk of sudden cardiac death. Beta-adrenergic blockers are the mainstay of treatment for LQTS. While their efficacy has been demonstrated in LQTS patients harbouring potassium channel mutations, studies of beta-blockers in subtype 3 (LQT3), which is caused by sodium channel mutations, have produced ambiguous results. In this modelling study, we explore the effects of beta-adrenergic drugs on the LQT3 phenotype.
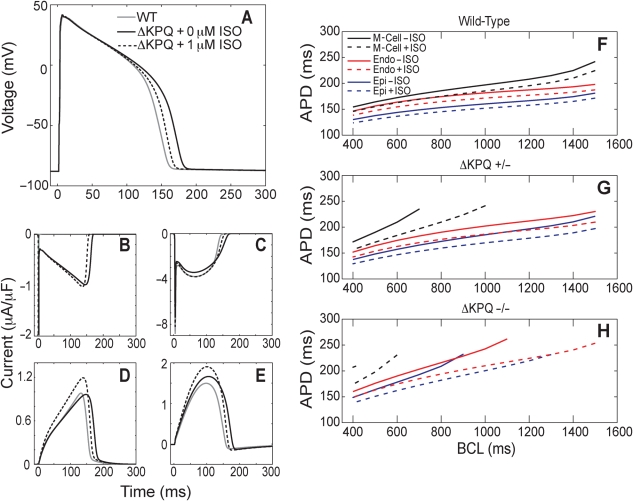
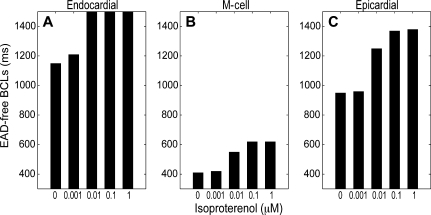
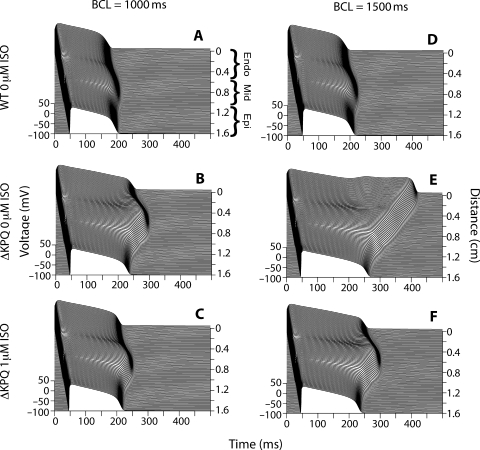
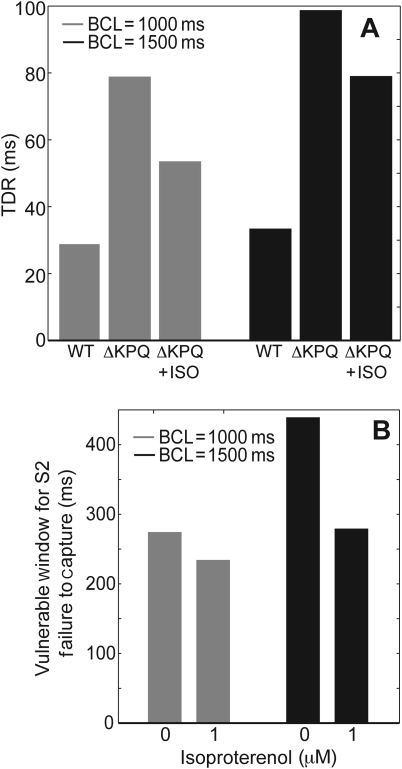
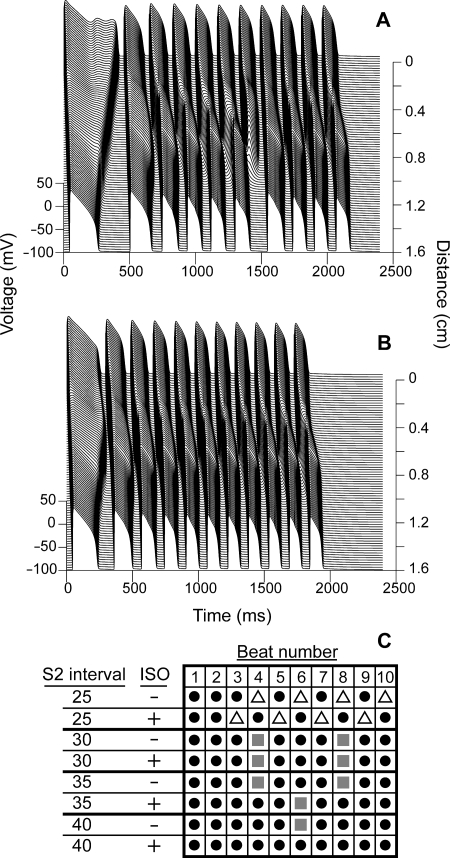
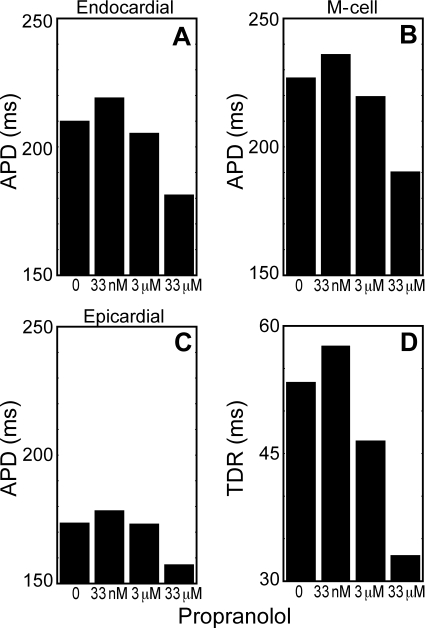
Methods and results: In order to investigate the effects of beta-adrenergic activity and to identify sources of ambiguity in earlier studies, we developed a computational model incorporating the effects of beta-agonists and beta-blockers into an LQT3 mutant guinea pig ventricular myocyte model. Beta-activation suppressed two arrhythmogenic phenomena, transmural dispersion of repolarization and early after depolarizations, in a dose-dependent manner. However, the ability of beta-activation to prevent cardiac conduction block was pacing-rate-dependent. Low-dose beta-blockade by propranolol reversed the beneficial effects of beta-activation, while high dose (which has off-target sodium channel effects) decreased arrhythmia susceptibility.
Conclusion: These results demonstrate that beta-activation may be protective in LQT3 and help to reconcile seemingly conflicting results from different experimental models. They also highlight the need for well-controlled clinical investigations re-evaluating the use of beta-blockers in LQT3 patients.
Figures
References
-
- Schwartz PJ, Locati EH, Moss AJ, Crampton RS, Trazzi R, Ruberti U. Left cardiac sympathetic denervation in the therapy of congenital long QT syndrome. A worldwide report. Circulation. 1991;84:503–511. - PubMed
-
- Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C, et al. Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias. Circulation. 2001;103:89–95. - PubMed
-
- Shimizu W, Noda T, Takaki H, Kurita T, Nagaya N, Satomi K, et al. Epinephrine unmasks latent mutation carriers with LQT1 form of congenital long-QT syndrome. J Am Coll Cardiol. 2003;41:633–642. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Schwartz PJ, Crampton RS, Benhorin J, et al. Effectiveness and limitations of beta-blocker therapy in congenital long-QT syndrome. Circulation. 2000;101:616–623. - PubMed
-
- Priori SG, Napolitano C, Schwartz PJ, Grillo M, Bloise R, Ronchetti E, et al. Association of long QT syndrome loci and cardiac events among patients treated with beta-blockers. JAMA. 2004;292:1341–1344. - PubMed
