

Uncharted paths: hospital networks in critical care
- PMID: 19265091
- PMCID: PMC2692049
- DOI: 10.1378/chest.08-1052
Uncharted paths: hospital networks in critical care
Abstract
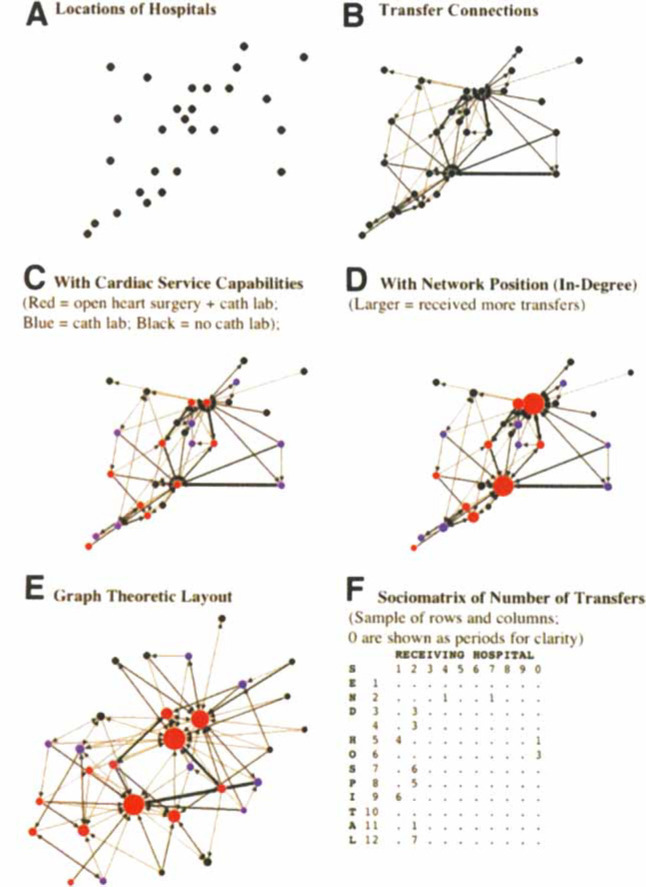
Wide variation between hospitals in the quality of critical care lead to many potentially avoidable deaths. Regionalization of critical care is a possible solution; regionalization has been implemented for trauma and neonatal intensive care, and it is under active discussion for medical and cardiac critical care. However, regionalization is only one possible approach to reorganizing critical care services. This commentary introduces the technique of network analysis as a framework for the following: (1) understanding how critically ill patients move between hospitals, (2) defining the roles hospitals play in regional care delivery, and (3) suggesting systematic improvements that may benefit population health. We examined transfers of critically ill Medicare patients in Connecticut in 2005 as a model system. We found that patients are systematically transferred to more capable hospitals. However, we find the standard distinction of hospitals into either "secondary hospitals" or "tertiary hospitals" poorly explains observed transfer patterns; instead, hospitals show a continuum of roles. We further examine the implications of the network pattern in a simulation of quarantine of a hospital to incoming transfers, as occurred during the severe acute respiratory syndrome epidemic. Network perspectives offer new ways to study systems to care for critically ill patients and provide additional tools for addressing pragmatic problems in triage and bed management, regionalization, quality improvement, and disaster preparedness.
Figures
References
-
- Barnato AE, Kahn JM, Rubenfeld GD. Prioritizing the Organization and Management of Intensive Care Services in the United States: the PrOMIS Conference. Crit Care Med. 2007;35:1003–1006. - PubMed
-
- Hannan EL. Evaluating and improving the quality of care for acute myocardial infarction: can regionalization help? JAMA. 2006;295:2177–2179. - PubMed
-
- University Healthsystem Consortium . Adult ICU Benchmarking Project: findings and conclusions. University Healthsystem Consortium; Oak Brook, IL: 2003.
-
- Pronovost PJ, Needham DM, Berenholtz SM. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355:2725–2732. - PubMed
-
- Krumholz HM, Wang Y, Mattera JA. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with an acute myocardial infarction. Circulation. 2006;113:1683–1692. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
