

Villitis of unknown etiology is associated with a distinct pattern of chemokine up-regulation in the feto-maternal and placental compartments: implications for conjoint maternal allograft rejection and maternal anti-fetal graft-versus-host disease
- PMID: 19265171
- PMCID: PMC2754231
- DOI: 10.4049/jimmunol.0803834
Villitis of unknown etiology is associated with a distinct pattern of chemokine up-regulation in the feto-maternal and placental compartments: implications for conjoint maternal allograft rejection and maternal anti-fetal graft-versus-host disease
Abstract
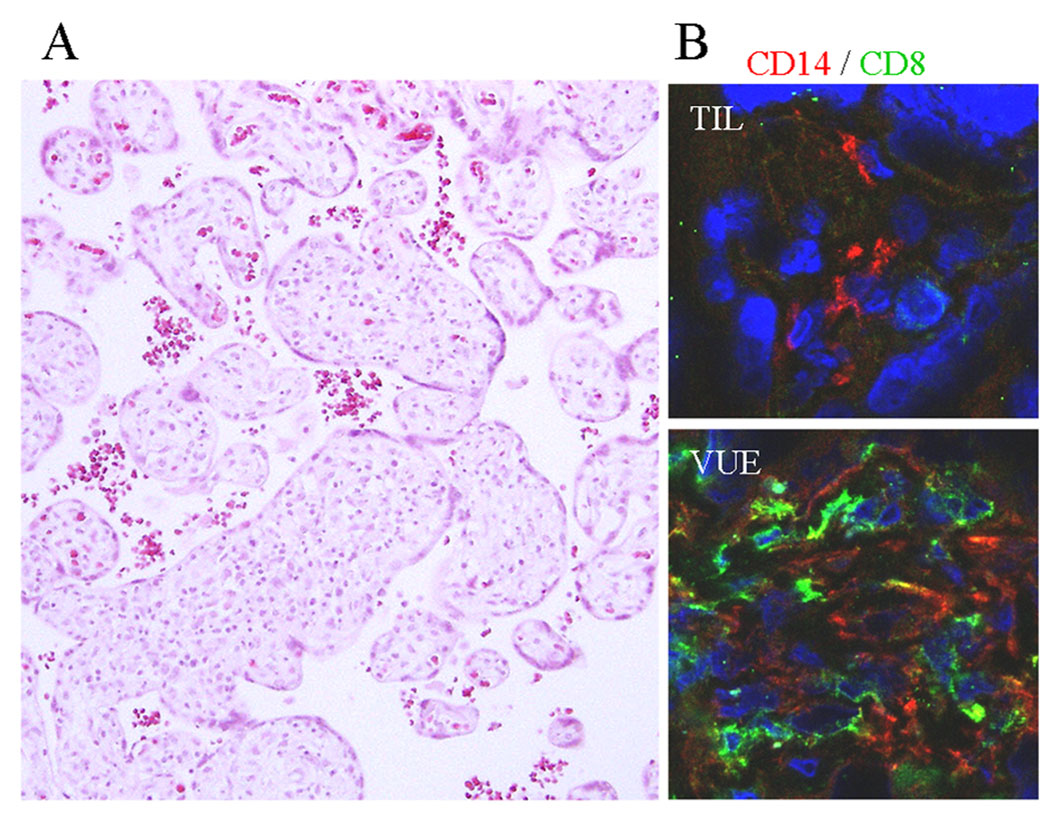
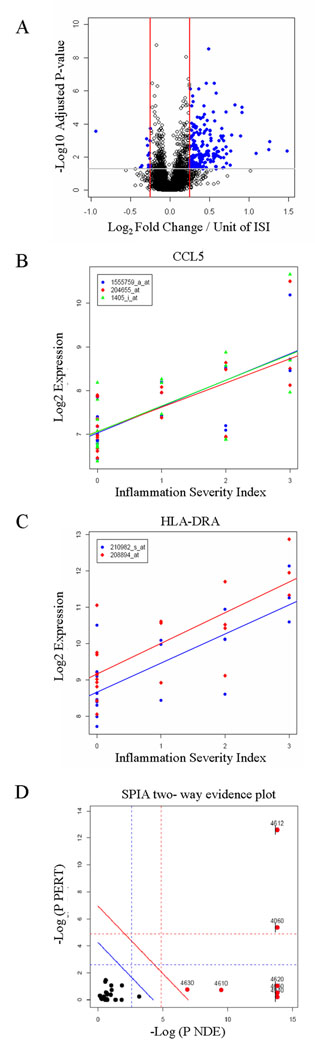
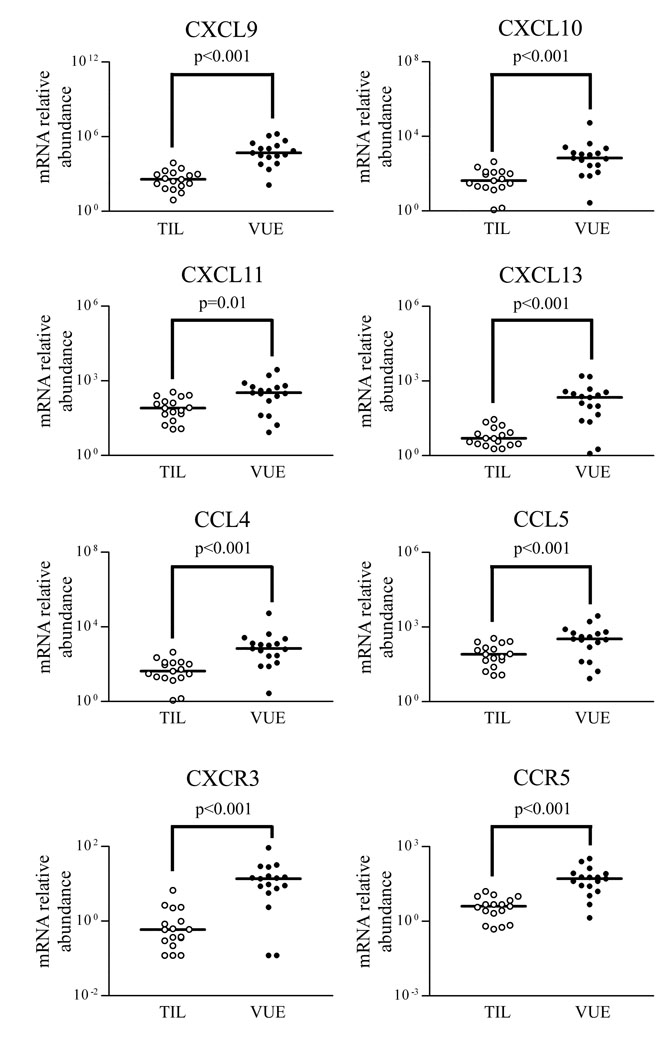
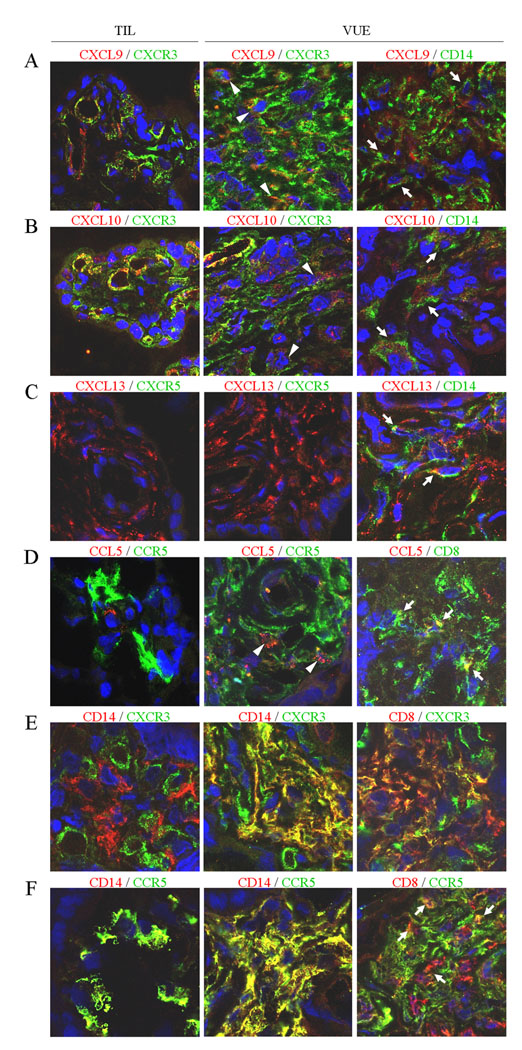
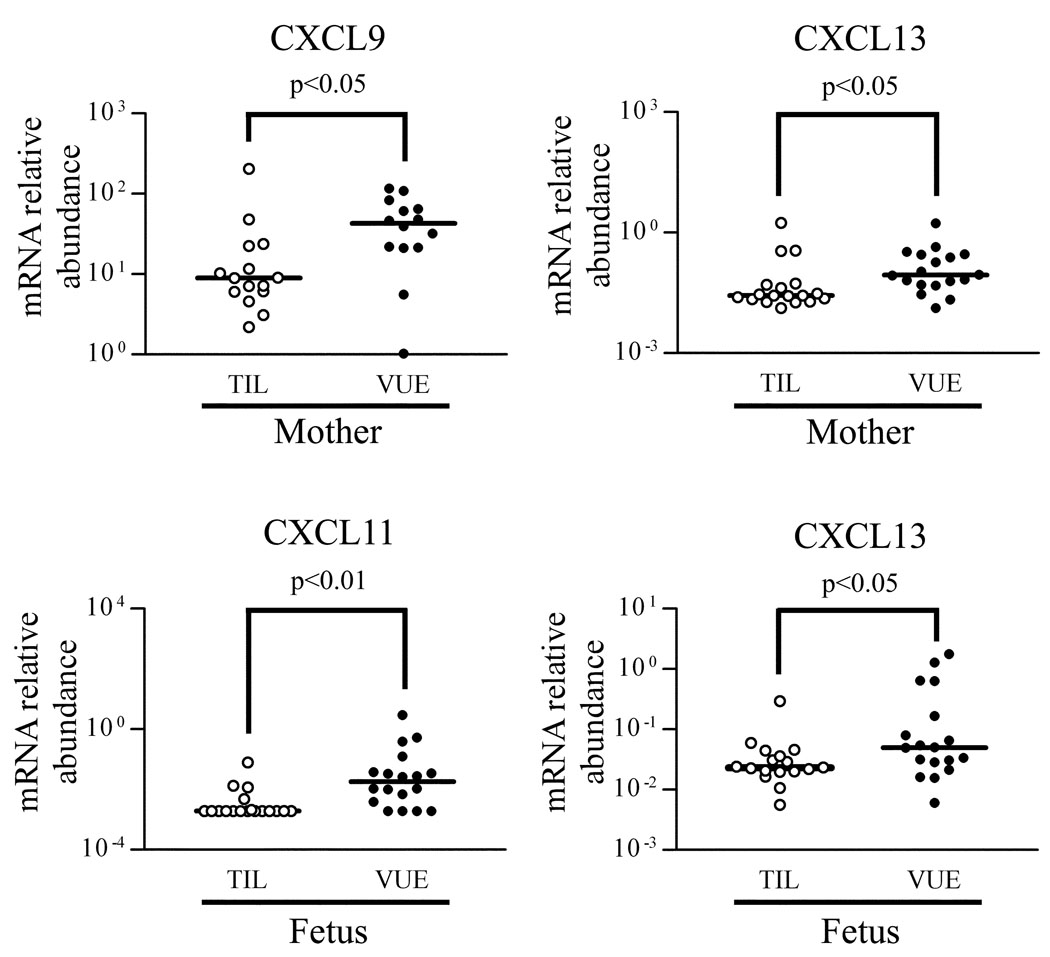
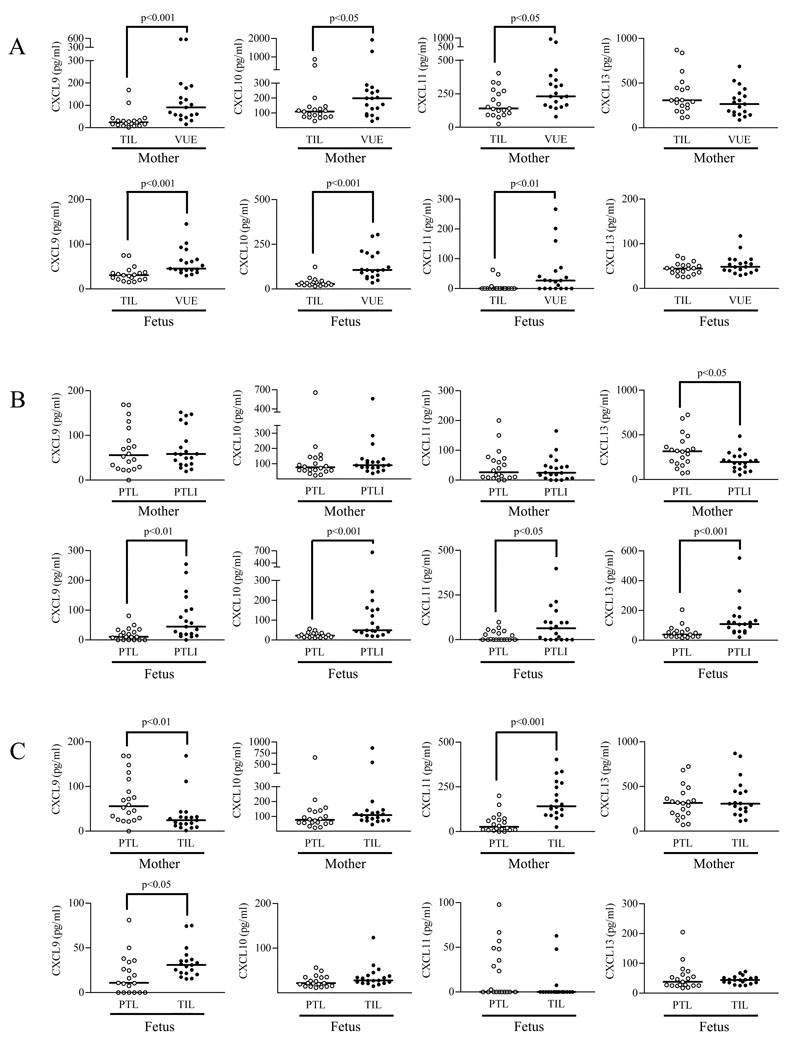
The co-presence of histoincompatible fetal and maternal cells is a characteristic of human placental inflammation. Villitis of unknown etiology (VUE), a destructive inflammatory lesion of villous placenta, is characterized by participation of Hofbauer cells (placental macrophages) and maternal T cells. In contrast to acute chorioamnionitis of infection-related origin, the fundamental immunopathology of VUE is unknown. This study was performed to investigate the placental transcriptome of VUE and to determine whether VUE is associated with systemic maternal and/or fetal inflammatory response(s). Comparison of the transcriptome between term placentas without and with VUE revealed differential expression of 206 genes associated with pathways related to immune response. The mRNA expression of a subset of chemokines and their receptors (CXCL9, CXCL10, CXCL11, CXCL13, CCL4, CCL5, CXCR3, CCR5) was higher in VUE placentas than in normal placentas (p < 0.05). Analysis of blood cell mRNA showed a higher expression of CXCL9 and CXCL13 in the mother, and CXCL11 and CXCL13 in the fetus of VUE cases (p < 0.05). The median concentrations of CXCL9, CXCL10, and CXCL11 in maternal and fetal plasma were higher in VUE (p < 0.05). Comparison of preterm cases without and with acute chorioamnionitis revealed elevated CXCL9, CXCL10, CXCL11, and CXCL13 concentrations in fetal plasma (p < 0.05), but not in maternal plasma with chorioamnionitis. We report for the first time the placental transcriptome of VUE. A systemic derangement of CXC chemokines in maternal and fetal circulation distinguishes VUE from acute chorioamnionitis. We propose that VUE be a unique state combining maternal allograft rejection and maternal antifetal graft-vs-host disease mechanisms.
Figures
References
-
- Kraus FT, Redline RW, Gersell DJ, Nelson DM, Diche JM. Inflammation and infection. In: Kraus FT, Redline RW, Gersell DJ, Nelson DM, Diche JM, editors. Placental Pathology Atlas of Non Tumor Pathology 3. 1st ed. Washington, DC: AFIP; 2004. pp. 75–116.
-
- Gomez R, Romero R, Ghezzi F, Yoon BH, Mazor M, Berry SM. The fetal inflammatory response syndrome. Am. J. Obstet. Gynecol. 1998;179:194–202. - PubMed
-
- Murtha AP, Greig PC, Jimmerson CE, Roitman-Johnson B, Allen J, Herbert WN. Maternal serum interleukin-6 concentrations in patients with preterm premature rupture of membranes and evidence of infection. Am. J. Obstet. Gynecol. 1996;175:966–969. - PubMed
-
- Shimoya K, Matsuzaki N, Taniguchi T, Okada T, Saji F, Murata Y. Interleukin-8 level in maternal serum as a marker for screening of histological chorioamnionitis at term. Int. J. Gynaecol. Obstet. 1997;57:153–159. - PubMed
-
- Brito H, Juliano P, Altemani C, Altemani A. Is the immunohistochemical study of the inflammatory infiltrate helpful in distinguishing villitis of unknown etiology from non-specific infection villitis? Placenta. 2005;26:839–841. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
