

Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis: consequences on haemodynamics, coagulation, acid-base status, and electrolytes
- PMID: 19265544
- PMCID: PMC2657128
- DOI: 10.1186/1471-2369-10-7
Citrate- vs. acetate-based dialysate in bicarbonate haemodialysis: consequences on haemodynamics, coagulation, acid-base status, and electrolytes
Abstract
Background: A concentrate for bicarbonate haemodialysis acidified with citrate instead of acetate has been marketed in recent years. The small amount of citrate used (one-fifth of the concentration adopted in regional anticoagulation) protects against intradialyser clotting while minimally affecting the calcium concentration. The aim of this study was to compare the impact of citrate- and acetate-based dialysates on systemic haemodynamics, coagulation, acid-base status, calcium balance and dialysis efficiency.
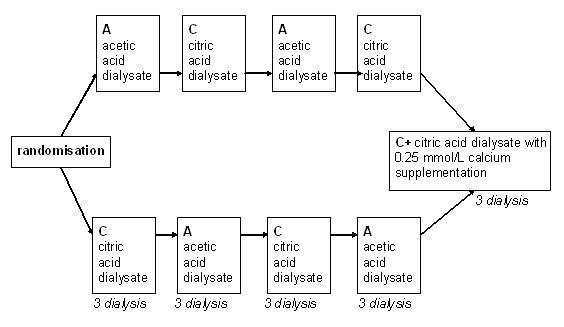
Methods: In 25 patients who underwent a total of 375 dialysis sessions, an acetate dialysate (A) was compared with a citrate dialysate with (C+) or without (C) calcium supplementation (0.25 mmol/L) in a randomised single-blind cross-over study. Systemic haemodynamics were evaluated using pulse-wave analysis. Coagulation, acid-base status, calcium balance and dialysis efficiency were assessed using standard biochemical markers.
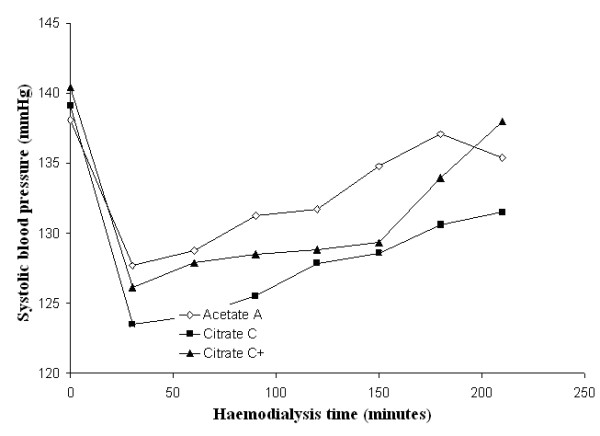
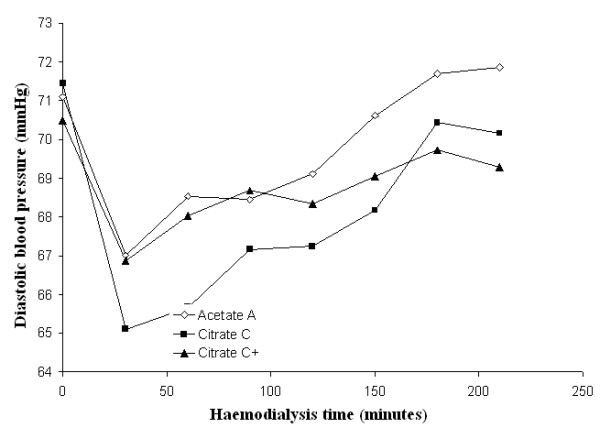
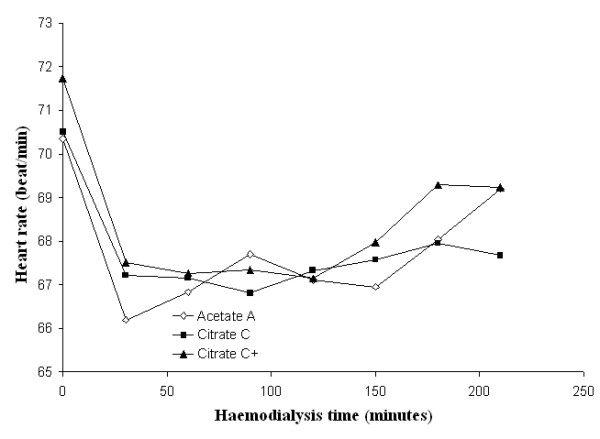
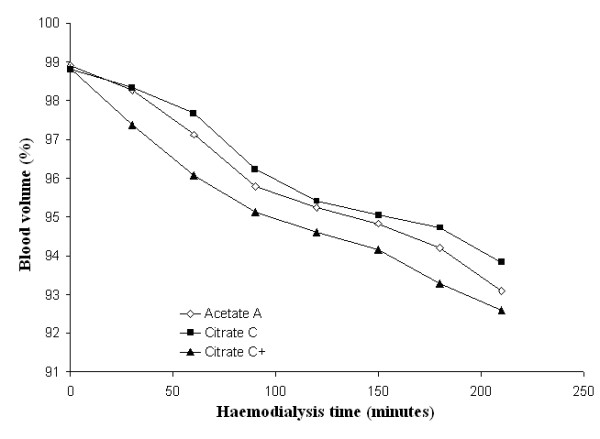
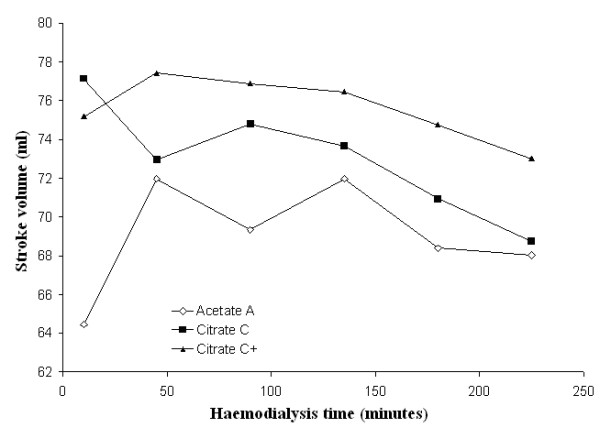
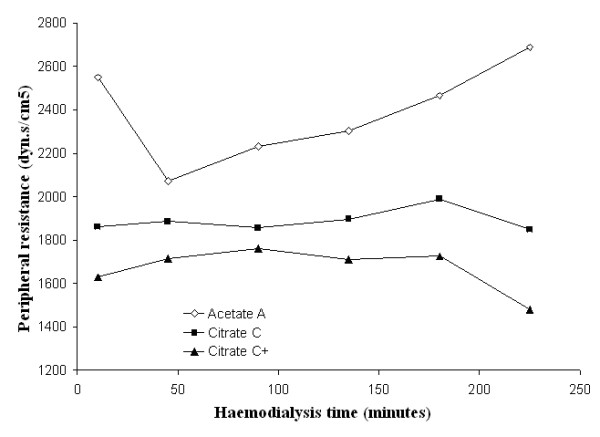
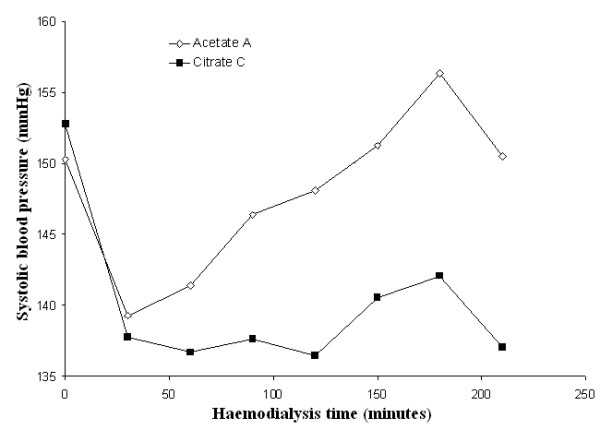
Results: Patients receiving the citrate dialysate had significantly lower systolic blood pressure (BP) (-4.3 mmHg, p < 0.01) and peripheral resistances (PR) (-51 dyne.sec.cm-5, p < 0.001) while stroke volume was not increased. In hypertensive patients there was a substantial reduction in BP (-7.8 mmHg, p < 0.01). With the C+ dialysate the BP gap was less pronounced but the reduction in PR was even greater (-226 dyne.sec.cm-5, p < 0.001). Analyses of the fluctuations in PR and of subjective tolerance suggested improved haemodynamic stability with the citrate dialysate. Furthermore, an increase in pre-dialysis bicarbonate and a decrease in pre-dialysis BUN, post-dialysis phosphate and ionised calcium were noted. Systemic coagulation activation was not influenced by citrate.
Conclusion: The positive impact on dialysis efficiency, acid-base status and haemodynamics, as well as the subjective tolerance, together indicate that citrate dialysate can significantly contribute to improving haemodialysis in selected patients.
Trial registration: ClinicalTrials.gov NCT00718289.
Figures
Similar articles
-
Comparative Effects of Acetate- and Citrate-Based Dialysates on Dialysis Dose and Protein-Bound Uremic Toxins in Hemodiafiltration Patients: Exploring the Impact of Calcium and Magnesium Concentrations.Toxins (Basel). 2024 Oct 1;16(10):426. doi: 10.3390/toxins16100426. Toxins (Basel). 2024. PMID: 39453202 Free PMC article.
-
Haemodynamic consequences of changing bicarbonate and calcium concentrations in haemodialysis fluids.Nephrol Dial Transplant. 2009 Mar;24(3):973-81. doi: 10.1093/ndt/gfn541. Epub 2008 Oct 8. Nephrol Dial Transplant. 2009. PMID: 18842671 Free PMC article. Clinical Trial.
-
Dialysate made from dry chemicals using citric acid increases dialysis dose.Am J Kidney Dis. 2000 Mar;35(3):493-9. doi: 10.1016/s0272-6386(00)70203-4. Am J Kidney Dis. 2000. PMID: 10692276 Clinical Trial.
-
Automated regional citrate anticoagulation: technological barriers and possible solutions.Blood Purif. 2010;29(2):204-9. doi: 10.1159/000245648. Epub 2010 Jan 8. Blood Purif. 2010. PMID: 20093828 Review.
-
Can regional anticoagulation with calcium-free dialysate be extended to maintenance hemodialysis?Artif Organs. 2024 Jul;48(7):704-712. doi: 10.1111/aor.14764. Epub 2024 May 8. Artif Organs. 2024. PMID: 38716639 Review.
Cited by
-
Increasing the Magnesium Concentration in Various Dialysate Solutions Differentially Modulates Oxidative Stress in a Human Monocyte Cell Line.Antioxidants (Basel). 2020 Apr 15;9(4):319. doi: 10.3390/antiox9040319. Antioxidants (Basel). 2020. PMID: 32326605 Free PMC article.
-
Citrate treatment reduces endothelial death and inflammation under hyperglycaemic conditions.Diab Vasc Dis Res. 2012 Jan;9(1):42-51. doi: 10.1177/1479164111424297. Epub 2011 Nov 1. Diab Vasc Dis Res. 2012. PMID: 22045866 Free PMC article.
-
Comparative Effects of Acetate- and Citrate-Based Dialysates on Dialysis Dose and Protein-Bound Uremic Toxins in Hemodiafiltration Patients: Exploring the Impact of Calcium and Magnesium Concentrations.Toxins (Basel). 2024 Oct 1;16(10):426. doi: 10.3390/toxins16100426. Toxins (Basel). 2024. PMID: 39453202 Free PMC article.
-
Conversion from acetate dialysate to citrate dialysate in a central delivery system for maintenance hemodialysis patients.Kidney Res Clin Pract. 2019 Mar 31;38(1):100-107. doi: 10.23876/j.krcp.18.0045. Kidney Res Clin Pract. 2019. PMID: 30754934 Free PMC article.
-
The effect of citrate dialysate on intradialytic heparin dose in haemodialysis patients: study design of a randomised controlled trial.BMC Nephrol. 2015 Aug 25;16:147. doi: 10.1186/s12882-015-0144-z. BMC Nephrol. 2015. PMID: 26303208 Free PMC article. Clinical Trial.
References
-
- Tu A, Ahmad S. Heparin-free hemodialysis with citrate-containing dialysate in intensive care patients. Neph Dial Transplant. 2000;29:620–626.
-
- Pinnick RV, Wiegmann TB, Diederich DA. Regional citrate anticoagulation for hemodialysis in the patient at high risk for bleeding. N Engl J Med. 1983;308:258–61. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
