

In-home particle concentrations and childhood asthma morbidity
- PMID: 19270802
- PMCID: PMC2649234
- DOI: 10.1289/ehp.11770
In-home particle concentrations and childhood asthma morbidity
Abstract
Background: Although outdoor particulate matter (PM) has been linked to mortality and asthma morbidity, the impact of indoor PM on asthma has not been well established.
Objective: This study was designed to investigate the effect of in-home PM on asthma morbidity.
Methods: For a cohort of 150 asthmatic children (2-6 years of age) from Baltimore, Maryland, a technician deployed environmental monitoring equipment in the children's bedrooms for 3-day intervals at baseline and at 3 and 6 months. Caregivers completed questionnaires and daily diaries during air sampling. Longitudinal data analyses included regression models with generalized estimating equations.
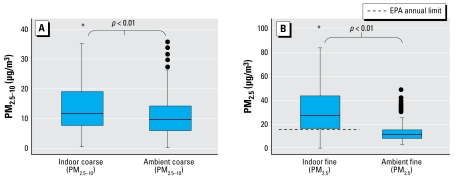
Results: Children were primarily African Americans (91%) from lower socioeconomic backgrounds and spent most of their time in the home. Mean (+/- SD) indoor PM(2.5-10) (PM with aerodynamic diameter 2.5-10 microm) and PM(2.5) (aerodynamic diameter < 2.5 microm) concentrations were 17.4 +/- 21.0 and 40.3 +/- 35.4 microg/m(3). In adjusted models, 10-microg/m(3) increases in indoor PM(2.5-10) and PM(2.5) were associated with increased incidences of asthma symptoms: 6% [95% confidence interval (CI), 1 to 12%] and 3% (95% CI, -1 to 7%), respectively; symptoms causing children to slow down: 8% (95% CI, 2 to 14%) and 4% (95% CI, 0 to 9%), respectively; nocturnal symptoms: 8% (95% CI, 1 to 14%) and 6% (95% CI, 1 to 10%), respectively; wheezing that limited speech: 11% (95% CI, 3 to 19%) and 7% (95% CI, 0 to 14%), respectively; and use of rescue medication: 6% (95% CI, 1 to 10%) and 4% (95% CI, 1 to 8%), respectively. Increases of 10 microg/m(3) in indoor and ambient PM(2.5) were associated with 7% (95% CI, 2 to 11%) and 26% (95% CI, 1 to 52%) increases in exercise-related symptoms, respectively.
Conclusions: Among preschool asthmatic children in Baltimore, increases in in-home PM(2.5-10) and PM(2.5) were associated with respiratory symptoms and rescue medication use. Increases in in-home and ambient PM(2.5) were associated with exercise-related symptoms. Although reducing PM outdoors may decrease asthma morbidity, reducing PM indoors, especially in homes of inner-city children, may lead to improved asthma health.
Keywords: air pollution; asthma; indoor; particulate matter; pediatric; urban.
Figures
References
-
- Allen R, Larson T, Sheppard L, Wallace L, Liu LS. Use of real-time light scattering data to estimate the contribution of infiltrated and indoor-generated particles to indoor air. Environ Sci Technol. 2003;37(16):3484–3492. - PubMed
-
- American Lung Association. State of Lung Disease in Diverse Communities. 2005. [[accessed 25 March 2008]]. Available: http://www.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=308853.
-
- Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, et al. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Respir J. 1995;8:483–491. - PubMed
-
- Asmussen L, Olson LM, Grant EN, Fagan J, Weiss KB. Reliability and validity of the Children’s Health Survey for Asthma. Pediatrics. 1999;104:e71. - PubMed
-
- Becker S, Mundandhara S, Devlin RB, Madden M. Regulation of cytokine production in human alveolar macrophages and airway epithelial cells in response to ambient air pollution particles: further mechanistic studies. Toxicol Appl Pharmacol. 2005;207:269–275. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
