

A cost-utility analysis of ablative therapy for Barrett's esophagus
- PMID: 19272389
- PMCID: PMC2693449
- DOI: 10.1053/j.gastro.2009.02.062
A cost-utility analysis of ablative therapy for Barrett's esophagus
Abstract
Background & aims: Recommendations for patients with Barrett's esophagus (BE) include endoscopic surveillance with esophagectomy for early-stage cancer, although new technologies to ablate dysplasia and metaplasia are available. This study compares the cost utility of ablation with that of endoscopic surveillance strategies.
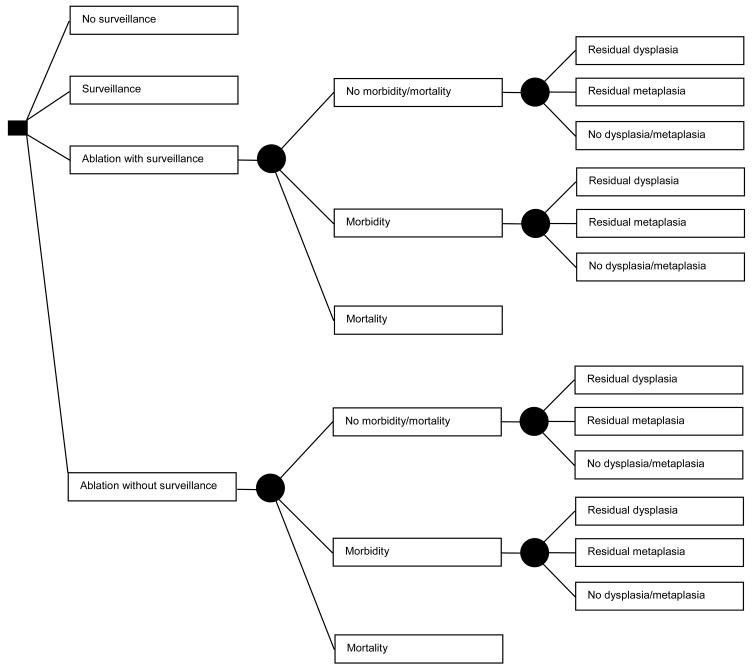
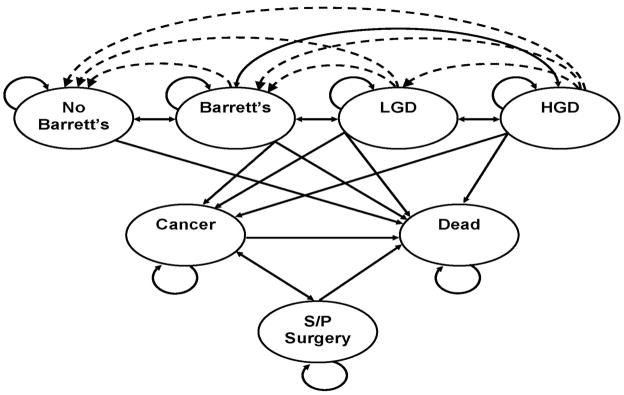
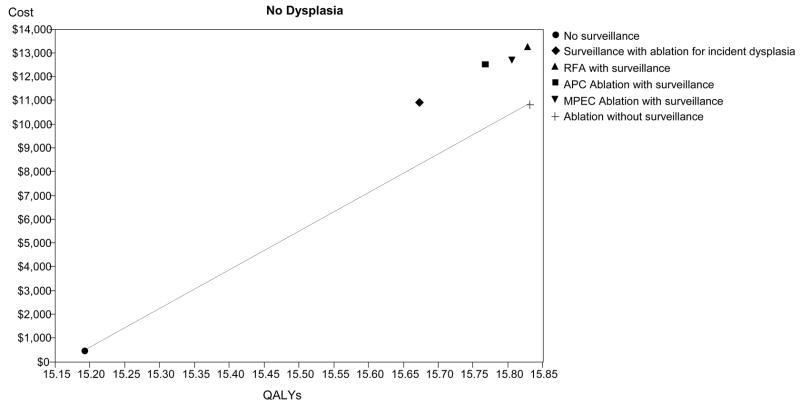
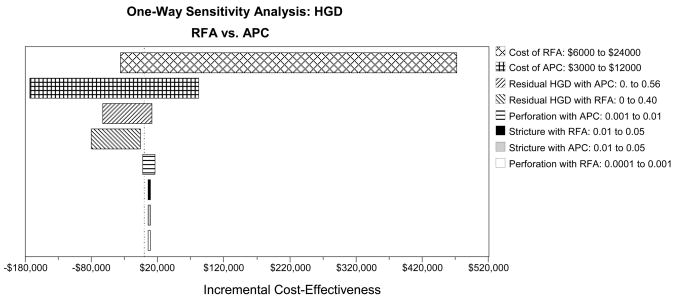
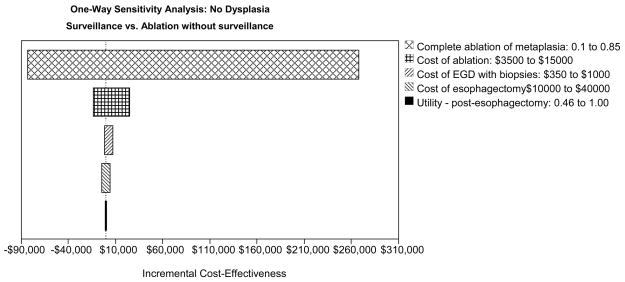
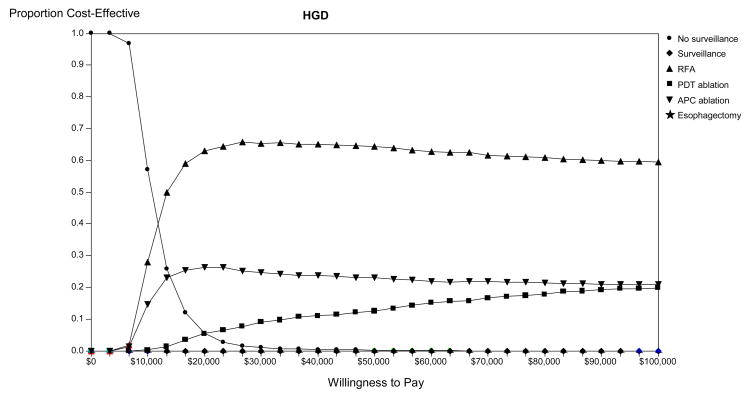
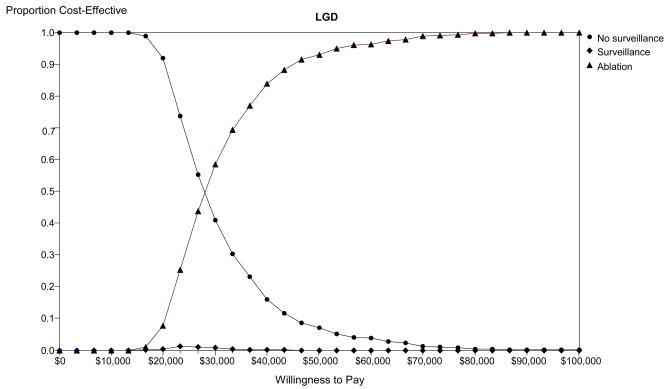
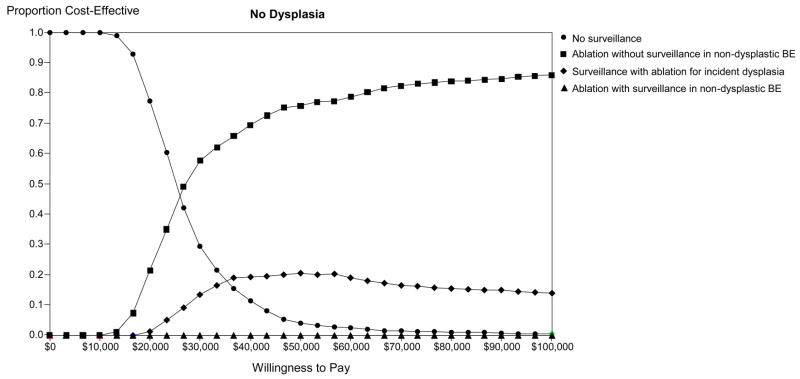
Methods: A decision analysis model was created to examine a population of patients with BE (mean age 50), with separate analyses for patients with no dysplasia, low-grade dysplasia (LGD), or high-grade dysplasia (HGD). Strategies compared were no endoscopic surveillance; endoscopic surveillance with ablation for incident dysplasia; immediate ablation followed by endoscopic surveillance in all patients or limited to patients in whom metaplasia persisted; and esophagectomy. Ablation modalities modeled included radiofrequency, argon plasma coagulation, multipolar electrocoagulation, and photodynamic therapy.
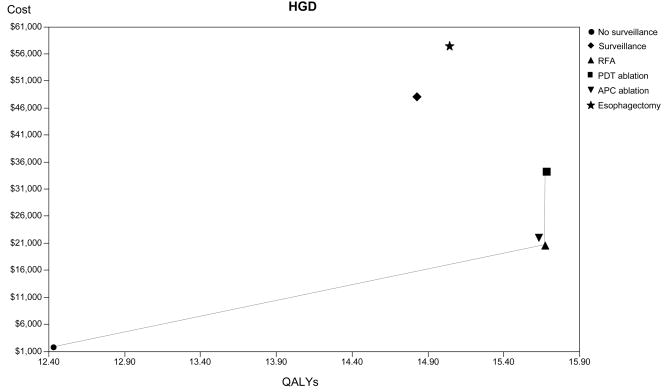
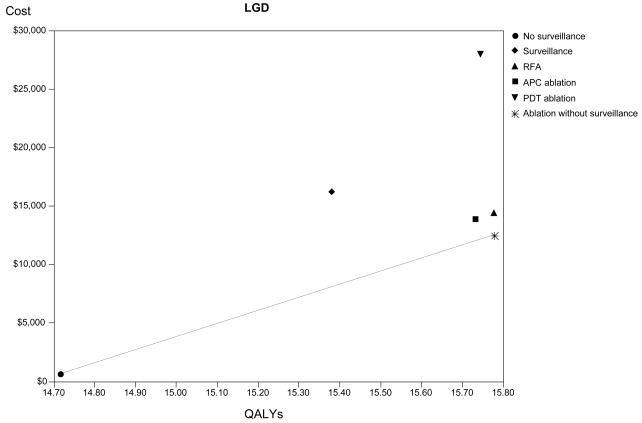
Results: Endoscopic ablation for patients with HGD could increase life expectancy by 3 quality-adjusted years at an incremental cost of <$6,000 compared with no intervention. Patients with LGD or no dysplasia can also be optimally managed with ablation, but continued surveillance after eradication of metaplasia is expensive. If ablation permanently eradicates >or=28% of LGD or 40% of nondysplastic metaplasia, ablation would be preferred to surveillance.
Conclusions: Endoscopic ablation could be the preferred strategy for managing patients with BE with HGD. Ablation might also be preferred in subjects with LGD or no dysplasia, but the cost effectiveness depends on the long-term effectiveness of ablation and whether surveillance endoscopy can be discontinued after successful ablation. As further postablation data become available, the optimal management strategy will be clarified.
Figures

References
-
- Lieberman DA, Oehlke M, Helfand M. Risk factors for Barrett’s esophagus in community-based practice. GORGE consortium. Gastroenterology Outcomes Research Group in Endoscopy. Am J Gastroenterol. 1997;92:1293–1297. - PubMed
-
- Wang KK, Sampliner RE. Updated Guidelines 2008 for the Diagnosis, Surveillance and Therapy of Barrett’s Esophagus. Am J Gastroenterol. 2008;103:788–797. - PubMed
-
- Wang KK, Wongkeesong M, Buttar NS. American Gastroenterological Association technical review on the role of the gastroenterologist in the management of esophageal carcinoma. Gastroenterology. 2005;128:1471–1505. - PubMed
-
- Wang KK, Wongkeesong M, Buttar NS. American Gastroenterological Association medical position statement: Role of the gastroenterologist in the management of esophageal carcinoma. Gastroenterology. 2005;128:1468–1470. - PubMed
-
- Shaheen NJ. Advances in Barrett’s esophagus and esophageal adenocarcinoma. Gastroenterology. 2005;128:1554–1566. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
