

Appendicitis, mesenteric lymphadenitis, and subsequent risk of ulcerative colitis: cohort studies in Sweden and Denmark
- PMID: 19273506
- PMCID: PMC2659291
- DOI: 10.1136/bmj.b716
Appendicitis, mesenteric lymphadenitis, and subsequent risk of ulcerative colitis: cohort studies in Sweden and Denmark
Abstract
Objective: To determine whether the repeatedly observed low risk of ulcerative colitis after appendicectomy is related to the appendicectomy itself or the underlying morbidity, notably appendicitis or mesenteric lymphadenitis.
Design: Nationwide cohort studies.
Setting: Sweden and Denmark.
Participants: 709 353 Swedish (1964-2004) and Danish (1977-2004) patients who had undergone appendicectomy were followed up for subsequent ulcerative colitis. The impact of appendicectomy on risk was also studied in 224 483 people whose parents or siblings had inflammatory bowel disease.
Main outcome measures: Standardised incidence ratios and rate ratios as measures of relative risk.
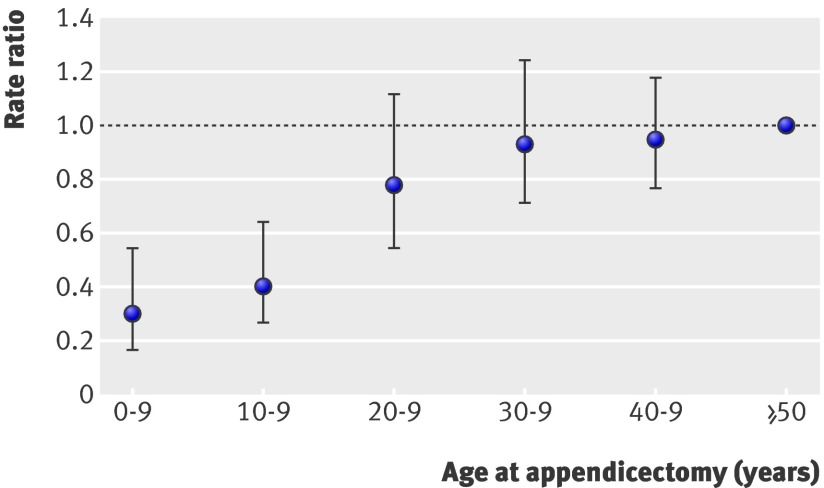
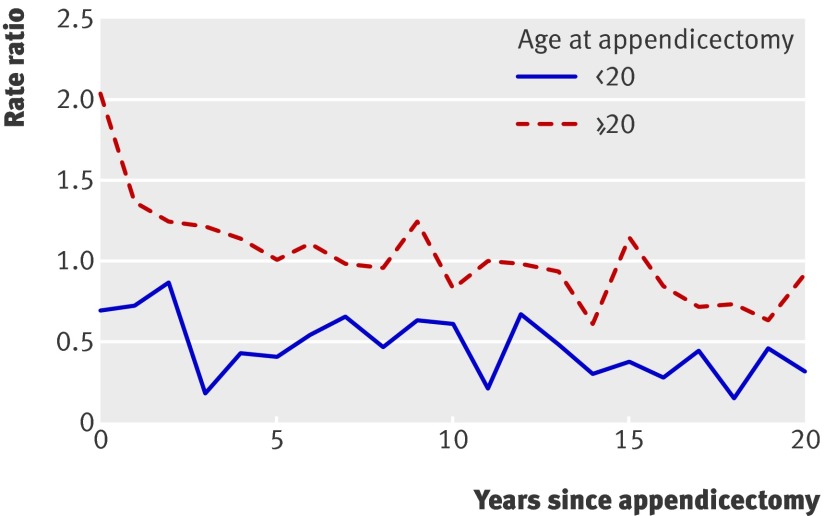
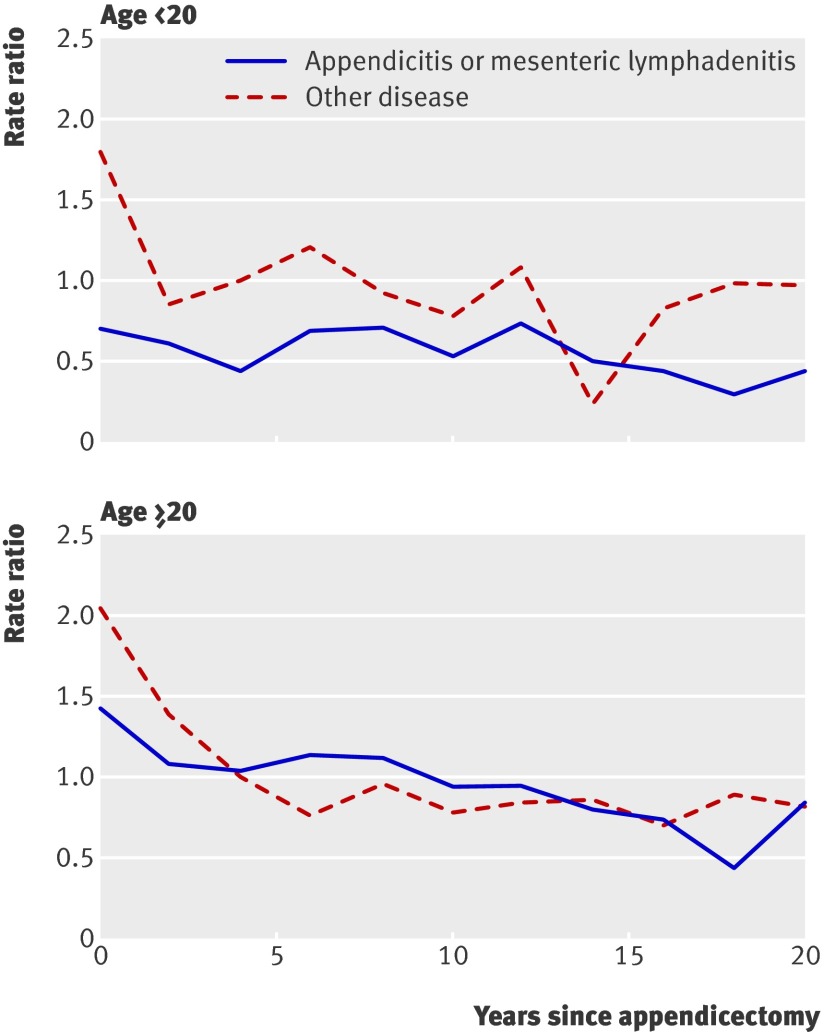
Results: During 11.1 million years of follow-up in the appendicectomy cohort, 1192 patients developed ulcerative colitis (10.8 per 100 000 person years). Appendicectomy without underlying inflammation was not associated with reduced risk (standardised incidence ratio 1.04, 95% confidence interval 0.95 to 1.15). Before the age of 20, however, appendicectomy for appendicitis (0.45, 0.39 to 0.53) or mesenteric lymphadenitis (0.65, 0.46 to 0.90) was associated with significant risk reduction. A similar pattern was seen in those with affected relatives, whose overall risk of ulcerative colitis was clearly higher than the background risk (1404 observed v 446 expected; standardised incidence ratio 3.15, 2.99 to 3.32). In this cohort, appendicectomy without underlying appendicitis did not modify risk (rate ratio 1.04, 0.66 to 1.55, v no appendicectomy), while risk after appendicectomy for appendicitis was halved (0.49, 0.31 to 0.74).
Conclusions: In individuals with or without a familial predisposition to inflammatory bowel disease, appendicitis and mesenteric lymphadenitis during childhood or adolescence are linked to a significantly reduced risk of ulcerative colitis in adulthood. Appendicectomy itself does not protect against ulcerative colitis.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Reduced risk of ulcerative colitis after appendicectomy.BMJ. 2009 Mar 9;338:b225. doi: 10.1136/bmj.b225. BMJ. 2009. PMID: 19273505 No abstract available.
-
Appendicitis, not appendectomy, is protective against ulcerative colitis, both in the general population and first-degree relatives of patients with IBD.Inflamm Bowel Dis. 2010 Feb;16(2):356-7. doi: 10.1002/ibd.21064. Inflamm Bowel Dis. 2010. PMID: 19685454 No abstract available.
References
-
- Podolsky DK. Inflammatory bowel disease. N Engl J Med 2002;347:417-29. - PubMed
-
- Koutroubakis IE, Vlachonikolis IG, Kouroumalis EA. Role of appendicitis and appendectomy in the pathogenesis of ulcerative colitis: a critical review. Inflamm Bowel Dis 2002;8:277-86. - PubMed
-
- Andersson RE, Olaison G, Tysk C, Ekbom A. Appendectomy and protection against ulcerative colitis. N Engl J Med 2001;344:808-14. - PubMed
-
- Frisch M, Johansen C, Mellemkjær L, Engels EA, Gridley G, Biggar RJ, et al. Appendectomy and subsequent risk of inflammatory bowel diseases. Surgery 2001;130:36-43. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical