

Microsatellite instability predicts improved response to adjuvant therapy with irinotecan, fluorouracil, and leucovorin in stage III colon cancer: Cancer and Leukemia Group B Protocol 89803
- PMID: 19273709
- PMCID: PMC2668707
- DOI: 10.1200/JCO.2008.18.2071
Microsatellite instability predicts improved response to adjuvant therapy with irinotecan, fluorouracil, and leucovorin in stage III colon cancer: Cancer and Leukemia Group B Protocol 89803
Abstract
Purpose: Colon cancers exhibiting DNA mismatch repair (MMR) defects demonstrate distinct clinical and pathologic features, including better prognosis and reduced response to fluorouracil (FU) -based chemotherapy. This prospective study investigated adjuvant chemotherapy containing FU and irinotecan in patients with MMR deficient (MMR-D) colon cancers.
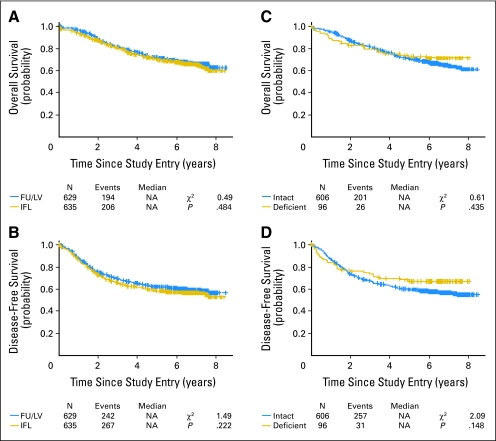
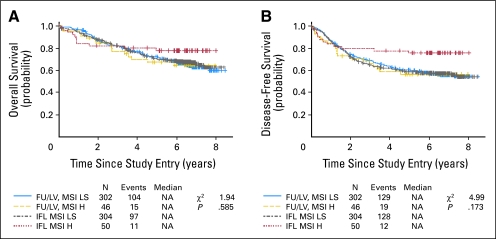
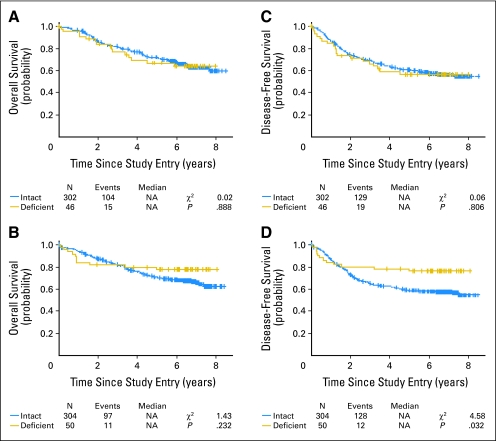
Patients and methods: Cancer and Leukemia Group B 89803 randomly assigned 1,264 patients with stage III colon cancer to postoperative weekly bolus FU/leucovorin (LV) or weekly bolus irinotecan, FU, and LV (IFL). The primary end point was overall survival; disease-free survival (DFS) was a secondary end point. Tumor expression of the MMR proteins, MLH1 and MSH2, was determined by immunohistochemistry (IHC). DNA microsatellite instability was also assessed using a panel of mono- and dinucleotide markers. Tumors with MMR defects were those demonstrating loss of MMR protein expression (MMR-D) and/or microsatellite instability high (MSI-H) genotype.
Results: Of 723 tumor cases examined by genotyping and IHC, 96 (13.3%) were MMR-D/MSI-H. Genotyping results were consistent with IHC in 702 cases (97.1%). IFL-treated patients with MMR-D/MSI-H tumors showed improved 5-year DFS as compared with those with mismatch repair intact tumors (0.76; 95% CI, 0.64 to 0.88 v 0.59; 95% CI, 0.53 to 0.64; P = .03). This relationship was not observed among patients treated with FU/LV. A trend toward longer DFS was observed in IFL-treated patients with MMR-D/MSI-H tumors as compared with those receiving FU/LV (0.57; 95% CI, 0.42 to 0.71 v 0.76; 95% CI, 0.64 to 0.88; P = .07; hazard ratio interaction between tumor status and treatment, 0.51; likelihood ratio P = .117).
Conclusion: Loss of tumor MMR function may predict improved outcome in patients treated with the IFL regimen as compared with those receiving FU/LV.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures

References
-
- Lengauer C, Kinzler KW, Vogelstein B. Genetic instability in colorectal cancers. Nature. 1997;386:623–627. - PubMed
-
- Perucho M. Cancer of the microsatellite mutator phenotype. Biol Chem. 1996;377:675–684. - PubMed
-
- Parsons R, Myeroff LL, Liu B, et al. Microsatellite instability and mutations of the transforming growth factor beta type II receptor gene in colorectal cancer. Cancer Res. 1995;58:5548–5557. - PubMed
-
- Rampino N, Yamamoto H, Ionov Y, et al. Somatic frameshift mutations in the BAX gene in colon cancers of microsatellite mutator phenotype. Science. 1997;275:967–969. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
