

DPC4 gene status of the primary carcinoma correlates with patterns of failure in patients with pancreatic cancer
- PMID: 19273710
- PMCID: PMC2668706
- DOI: 10.1200/JCO.2008.17.7188
DPC4 gene status of the primary carcinoma correlates with patterns of failure in patients with pancreatic cancer
Abstract
Purpose: Contrary to the extensive data accumulated regarding pancreatic carcinogenesis, the clinical and molecular features characteristic of advanced stage (stage III and IV) disease are unknown. A comprehensive study of pancreatic cancers from patients who have succumbed to their disease has the potential to greatly expand our understanding of the most lethal stage of this disease and identify novel areas for intervention.
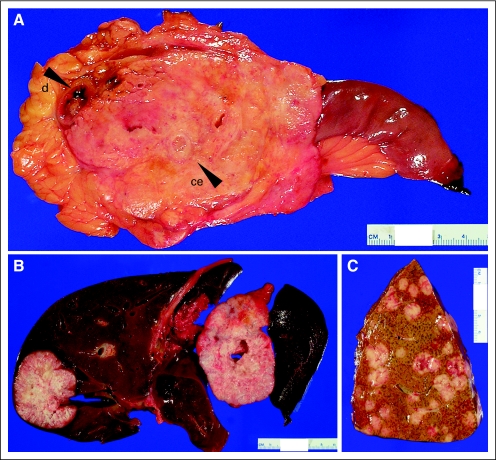
Materials and methods: Rapid autopsies were performed on 76 patients with documented pancreatic cancer. The histologic features of end stage disease were determined and correlated to the stage at initial diagnosis, patterns of failure (locally destructive v metastatic disease) and the status of the KRAS2, TP53, and DPC4 genes.
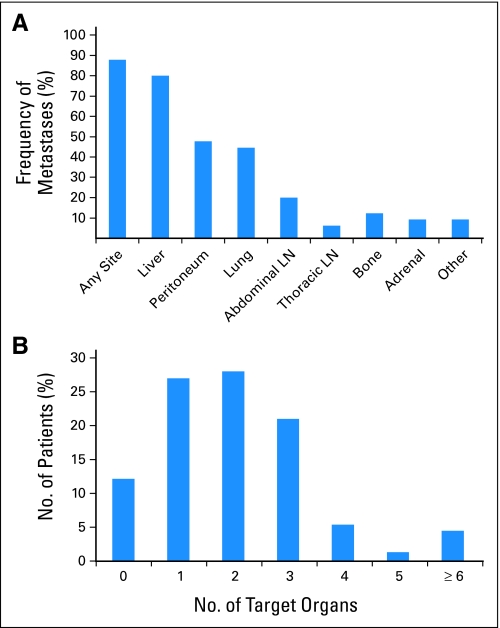
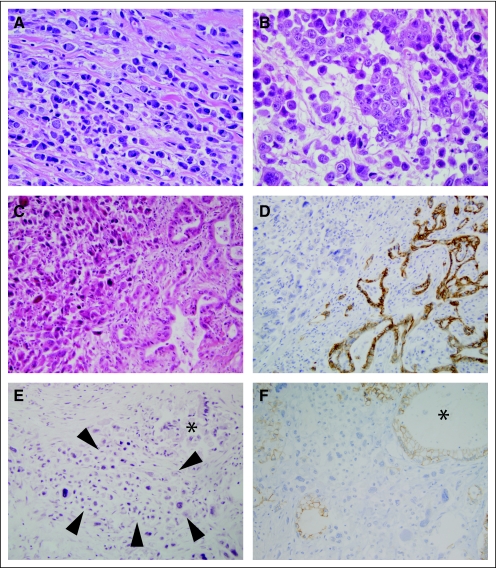
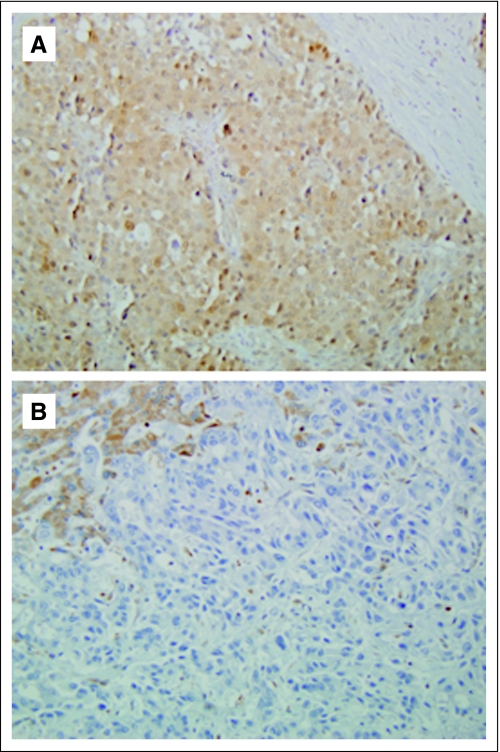
Results: At autopsy, 30% of patients died with locally destructive pancreatic cancer, and 70% died with widespread metastatic disease. These divergent patterns of failure found at autopsy (locally destructive v metastatic) were unrelated to clinical stage at initial presentation, treatment history, or histopathologic features. However, Dpc4 immunolabeling status of carcinoma tissues harvested at autopsy, a sensitive marker of DPC4 genetic status, was highly correlated with the presence of widespread metastasis but not with locally destructive tumors (P = .007).
Conclusion: Pancreatic cancers are represented by distinct genetic subtypes with significantly different patterns of failure. Determinations of DPC4 status at initial diagnosis may be of value in stratifying patients into treatment regimens related to local control versus systemic therapy.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Role of radiation therapy in the management of locally advanced pancreatic cancer.J Clin Oncol. 2012 May 1;30(13):1564-5; author reply 1566-7. doi: 10.1200/JCO.2011.40.8674. Epub 2012 Mar 12. J Clin Oncol. 2012. PMID: 22412127 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinoma of the pancreas-616 patients: Results, outcomes, and prognostic indicators. J Gastrointest Surg. 2000;4:567–579. - PubMed
-
- Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg. 2006;10:1199–1210. discussion 1210-1211, 2006. - PubMed
-
- Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: A phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25:1960–1966. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
