

Health care costs in the last week of life: associations with end-of-life conversations
- PMID: 19273778
- PMCID: PMC2862687
- DOI: 10.1001/archinternmed.2008.587
Health care costs in the last week of life: associations with end-of-life conversations
Abstract
Background: Life-sustaining medical care of patients with advanced cancer at the end of life (EOL) is costly. Patient-physician discussions about EOL wishes are associated with lower rates of intensive interventions.
Methods: Funded by the National Institute of Mental Health and the National Cancer Institute, Coping With Cancer is a longitudinal multi-institutional study of 627 patients with advanced cancer. Patients were interviewed at baseline and were followed up through death. Costs for intensive care unit and hospital stays, hospice care, and life-sustaining procedures (eg, mechanical ventilator use and resuscitation) received in the last week of life were aggregated. Generalized linear models were applied to test for cost differences in EOL care. Propensity score matching was used to reduce selection biases.
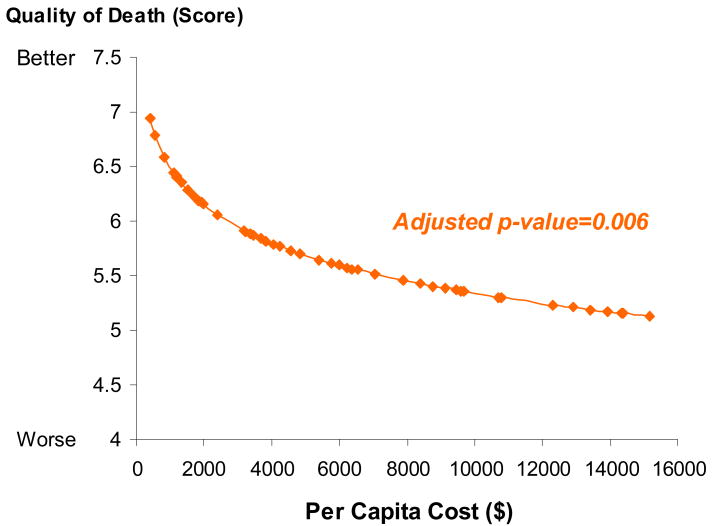
Results: Of 603 participants, 188 (31.2%) reported EOL discussions at baseline. After propensity score matching, the remaining 415 patients did not differ in sociodemographic characteristics, recruitment sites, illness acknowledgment, or treatment preferences. Further analyses, adjusted by quintiles of propensity scores and significant confounders, revealed that the mean (SE) aggregate costs of care (in 2008 US dollars) were $1876 ($177) for patients who reported EOL discussions compared with $2917 ($285) for patients who did not, a cost difference of $1041 (35.7% lower among patients who reported EOL discussions) (P =.002). Patients with higher costs had worse quality of death in their final week (Pearson production moment correlation partial r = -0.17, P =.006).
Conclusions: Patients with advanced cancer who reported having EOL conversations with physicians had significantly lower health care costs in their final week of life. Higher costs were associated with worse quality of death.
Figures
Comment in
-
Life prolonging in name only?Arch Intern Med. 2009 Sep 14;169(16):1540; author reply 1540-1. doi: 10.1001/archinternmed.2009.273. Arch Intern Med. 2009. PMID: 19752418 No abstract available.
References
-
-
Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group, 2006 National Health Care Expenditures Data, January 2008.
-
-
- Emanuel Ezekiel J, Ash Arlene, Yu Wei, Gazelle Gail, Levinsky Norman G, Saynina Olga, McClellan Mark, Moskowitz Mark. Managed care, hospice use, site of death, and medical expenditures in the last year of life. Archives of Internal Medicine. 2002 Aug 12/26;162 - PubMed
-
- Yu W. End of Life Care: Medical Treatments and Costs by Age, Race, and Region. HSR&D study IIR 02-189. URI: http://www.hsrd.research.va.gov/research/abstracts/IIR_02-189.htm.
-
- Wright Alexi A, Zhang Baohui, Ray Alaka, Mack Jennifer W, Trice Elizabeth, Balboni Tracy, Mitchell Susan L, Jackson Vicki A, Block Susan D, Maciejewski Paul K, Prigerson Holly G. Associations between end-of-1 life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. (resubmitted) - PMC - PubMed
