

Prevention of breast cancer in postmenopausal women: approaches to estimating and reducing risk
- PMID: 19276457
- PMCID: PMC2720698
- DOI: 10.1093/jnci/djp018
Prevention of breast cancer in postmenopausal women: approaches to estimating and reducing risk
Abstract
Background: It is uncertain whether evidence supports routinely estimating a postmenopausal woman's risk of breast cancer and intervening to reduce risk.
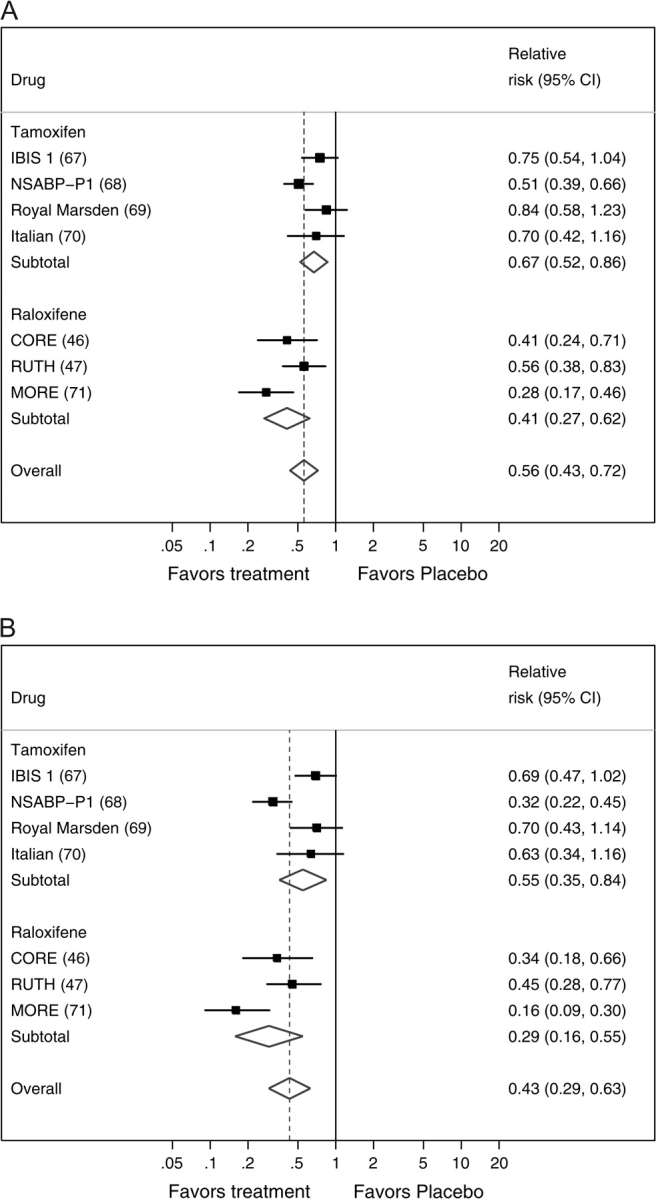
Methods: We systematically reviewed prospective studies about models and sex hormone levels to assess breast cancer risk and used meta-analysis with random effects models to summarize the predictive accuracy of breast density. We also reviewed prospective studies of the effects of exercise, weight management, healthy diet, moderate alcohol consumption, and fruit and vegetable intake on breast cancer risk, and used random effects models for a meta-analyses of tamoxifen and raloxifene for primary prevention of breast cancer. All studies reviewed were published before June 2008, and all statistical tests were two-sided.
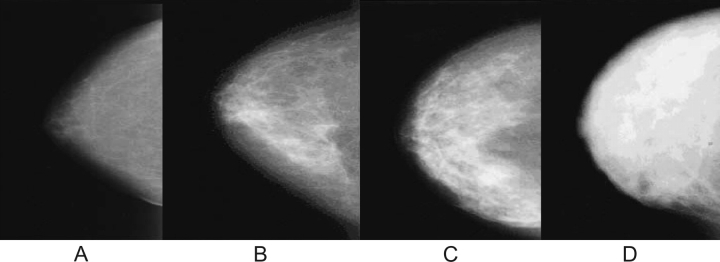
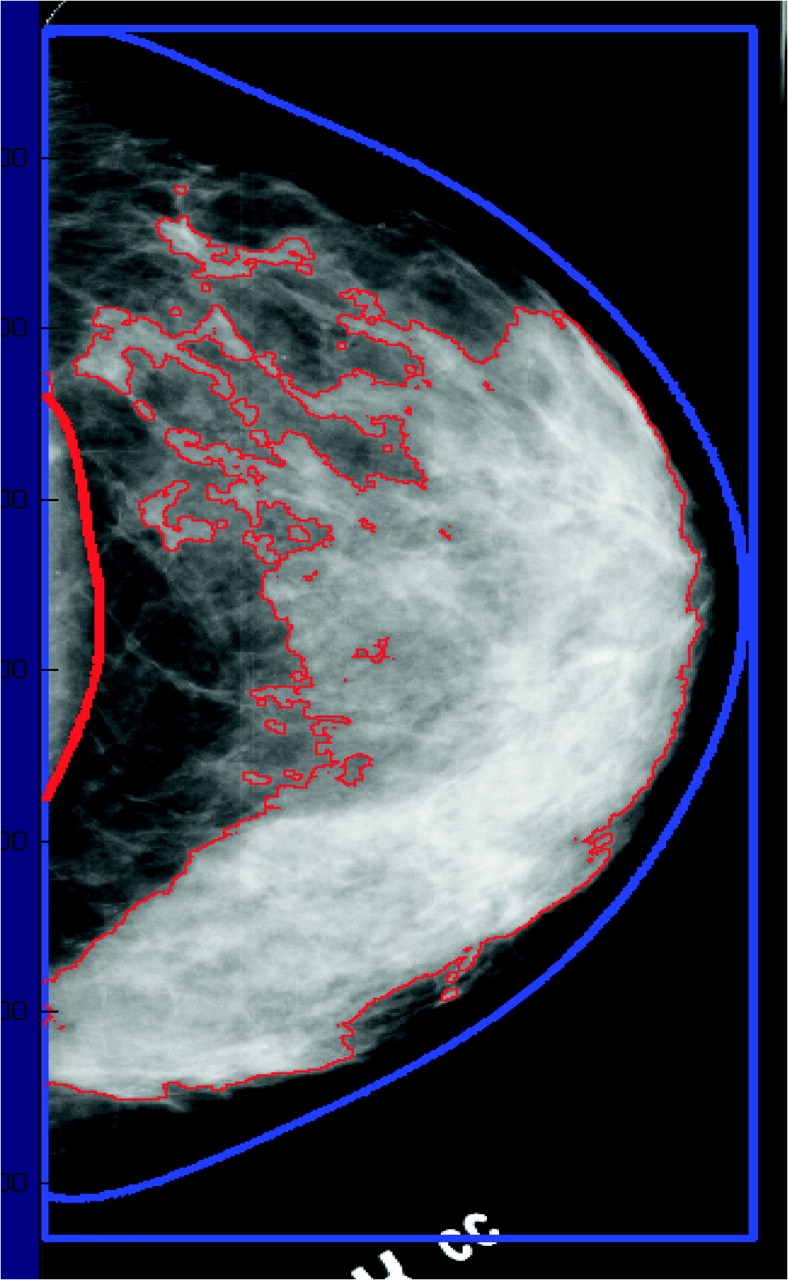
Results: Risk models that are based on demographic characteristics and medical history had modest discriminatory accuracy for estimating breast cancer risk (c-statistics range = 0.58-0.63). Breast density was strongly associated with breast cancer (relative risk [RR] = 4.03, 95% confidence interval [CI] = 3.10 to 5.26, for Breast Imaging Reporting and Data System category IV vs category I; RR = 4.20, 95% CI = 3.61 to 4.89, for >75% vs <5% of dense area), and adding breast density to models improved discriminatory accuracy (c-statistics range = 0.63-0.66). Estradiol was also associated with breast cancer (RR range = 2.0-2.9, comparing the highest vs lowest quintile of estradiol, P < .01). Most studies found that exercise, weight reduction, low-fat diet, and reduced alcohol intake were associated with a decreased risk of breast cancer. Tamoxifen and raloxifene reduced the risk of estrogen receptor-positive invasive breast cancer and invasive breast cancer overall.
Conclusions: Evidence from this study supports screening for breast cancer risk in all postmenopausal women by use of risk factors and breast density and considering chemoprevention for those found to be at high risk. Several lifestyle changes with the potential to prevent breast cancer should be recommended regardless of risk.
Figures
References
-
- American Cancer Society. Cancer Facts and Figures 2007. Atlanta, GA: American Cancer Society; 2007.
-
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137(5 pt 1):347–360. - PubMed
-
- US Preventive Services Task Force. Chemoprevention of breast cancer: recommendations and rationale. Ann Intern Med. 2002;137(1):56–58. - PubMed
-
- Kinsinger LS, Harris R, Woolf SH, Sox HC, Lohr KN. Chemoprevention of breast cancer: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137(1):59–69. - PubMed
-
- Chlebowski RT, Col N, Winer EP, et al. American Society of Clinical Oncology technology assessment of pharmacologic interventions for breast cancer risk reduction including tamoxifen, raloxifene, and aromatase inhibition. J Clin Oncol. 2002;20(15):3328–3343. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
