

The Minnesota Grading System using fundus autofluorescence of eye bank eyes: a correlation to age-related macular degeneration (an AOS thesis)
- PMID: 19277247
- PMCID: PMC2646441
The Minnesota Grading System using fundus autofluorescence of eye bank eyes: a correlation to age-related macular degeneration (an AOS thesis)
Abstract
Purpose: To establish a grading system of eye bank eyes using fundus autofluorescence (FAF) and identify a methodology that correlates FAF to age-related macular degeneration (AMD) with clinical correlation to the Age-Related Eye Disease Study (AREDS).
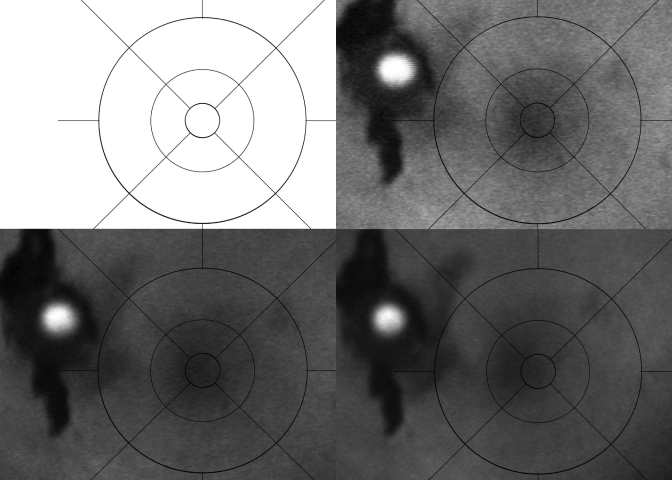
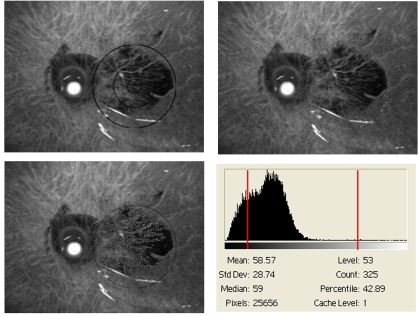
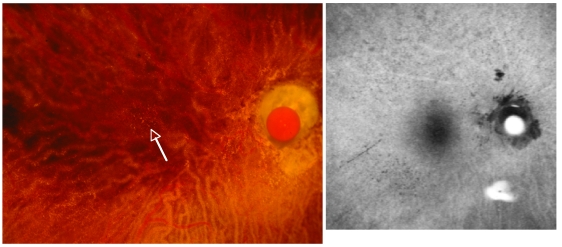
Methods: Two hundred sixty-two eye bank eyes were evaluated using a standardized analysis of FAF. Measurements were taken with the confocal scanning laser ophthalmoscope (cSLO). First, high-resolution, digital, stereoscopic, color images were obtained and graded according to AREDS criteria. With the neurosensory retina removed, mean FAF values were obtained from cSLO images using software analysis that excludes areas of atrophy and other artifact, generating an FAF value from a grading template. Age and AMD grade were compared to FAF values. An internal fluorescence reference standard was tested.
Results: Standardization of the cSLO machine demonstrated that reliable data could be acquired after a 1-hour warm-up. Images obtained prior to 1 hour had falsely elevated levels of FAF. In this initial analysis, there was no statistical correlation of age to mean FAF. There was a statistically significant decrease in FAF from AREDS grade 1, 2 to 3, 4 (P < .0001). An internal fluorescent standard may serve as a quantitative reference.
Conclusions: The Minnesota Grading System (MGS) of FAF (MGS-FAF) establishes a standardized methodology for grading eye bank tissue to quantify FAF compounds in the retinal pigment epithelium and correlate these findings to the AREDS. Future studies could then correlate specific FAF to the aging process, histopathology AMD phenotypes, and other maculopathies, as well as to analyze the biochemistry of autofluorescent fluorophores.
Figures








Similar articles
-
The Minnesota Grading System of eye bank eyes for age-related macular degeneration.Invest Ophthalmol Vis Sci. 2004 Dec;45(12):4484-90. doi: 10.1167/iovs.04-0342. Invest Ophthalmol Vis Sci. 2004. PMID: 15557458
-
The Age-Related Macular Degeneration Complex: Linking Epidemiology and Histopathology Using the Minnesota Grading System (The Inaugural Frederick C. Blodi Lecture).Trans Am Ophthalmol Soc. 2015 Sep;113:Blodi. Trans Am Ophthalmol Soc. 2015. PMID: 27895380 Free PMC article.
-
Comparison of fundus autofluorescence of age-related macular degeneration between a fundus camera and a confocal scanning laser ophthalmoscope.Osaka City Med J. 2009 Jun;55(1):19-27. Osaka City Med J. 2009. PMID: 19725431
-
The Use of Fundus Autofluorescence in Dry Age-Related Macular Degeneration.Turk J Ophthalmol. 2021 Jun 29;51(3):169-176. doi: 10.4274/tjo.galenos.2020.49107. Turk J Ophthalmol. 2021. PMID: 34187152 Free PMC article. Review.
-
Fundus autofluorescence imaging in age-related macular degeneration and geographic atrophy.Adv Exp Med Biol. 2010;664:395-402. doi: 10.1007/978-1-4419-1399-9_45. Adv Exp Med Biol. 2010. PMID: 20238040 Review.
Cited by
-
Enhanced Detection of Sub-Retinal Pigment Epithelial Cell Layer Deposits in Human and Murine Tissue: Imaging Zinc as a Biomarker for Age-Related Macular Degeneration (An American Ophthalmological Society Thesis).Trans Am Ophthalmol Soc. 2017 Aug 22;115:T3. eCollection 2017 Aug. Trans Am Ophthalmol Soc. 2017. PMID: 29021717 Free PMC article.
-
Histopathological assessments reveal retinal vascular changes, inflammation, and gliosis in patients with lethal COVID-19.Graefes Arch Clin Exp Ophthalmol. 2022 Apr;260(4):1275-1288. doi: 10.1007/s00417-021-05460-1. Epub 2021 Oct 29. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 34714382 Free PMC article.
References
-
- Buch H, Vinding T, La Cour M, Appleyard M, Jensen GB, Nielsen NV. Prevalence and causes of visual impairment and blindness among 9980 Scandinavian adults: The Copenhagen City Eye Study. Ophthalmology. 2004;111:53–61. - PubMed
-
- Buch H, Vinding T, Nielsen NV. Prevalence and causes of visual impairment according to World Health Organization and United States criteria in an aged, urban Scandinavian population: the Copenhagen City Eye Study. Ophthalmology. 2001;108:2347–2357. - PubMed
-
- Klaver CC, Wolfs RC, Vingerling JR, Hofman A, de Jong PT. Age-specific prevalence and causes of blindness and visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol. 1998;116:653–658. - PubMed
-
- O'Shea JG. Age-related macular degeneration: a leading cause of blindness [see comments] Med J Aust. 1996;165:561–564. - PubMed
-
- Mitchell P, Smith W, Attebo K, Wang JJ. Prevalence of age-related maculopathy in Australia. The Blue Mountains Eye Study. Ophthalmology. 1995;102:1450–1460. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
