

Arthroscopically assisted removal of intraosseous ganglion cysts of the distal tibia
- PMID: 19277804
- PMCID: PMC2758966
- DOI: 10.1007/s11999-009-0771-4
Arthroscopically assisted removal of intraosseous ganglion cysts of the distal tibia
Abstract
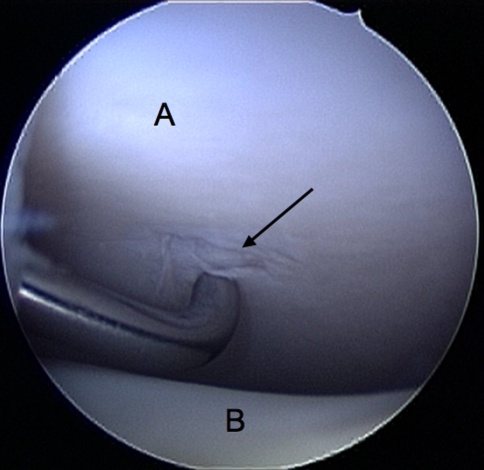
Intraosseous ganglia of the distal tibia are rare. We evaluated the feasibility of surgically treating these lesions with an arthroscopically assisted technique. Five patients with symptomatic distal tibial ganglia underwent surgical curettage and excision with this technique. All patients underwent débridement of the chondral lesion and hypertrophied synovial lining when present, probing of the portal to the ganglion, and subsequently thorough curettage with bone grafting performed through a cortical window made from a separate small incision. Biopsy confirmed the diagnosis in all patients. All patients had eventual relief of symptoms with good integration of bone graft at final followup. There were no recurrences at a minimum followup of 19 months (mean, 38.6 months; range, 19-69 months). Mean time for return to full function was 15.4 weeks (range, 8-17 weeks). There were no intraoperative or postoperative complications. The mean American Orthopaedic Foot and Ankle Society scores increased from 73 points (range, 67-77 points) preoperatively to 94 points (range, 90-100 points) postoperatively. Arthroscopically assisted surgical treatment of ganglia of the distal tibia in the appropriate patient is a reasonably simple technique that relieves symptoms and helps the patient to regain normal gait and full function with no recurrence (in our small series).
Level of evidence: Level IV, case series. See Guidelines for Authors for a complete description of levels of evidence.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
