

Endovascular approaches to acute stroke, part 1: Drugs, devices, and data
- PMID: 19279271
- PMCID: PMC7051752
- DOI: 10.3174/ajnr.A1486
Endovascular approaches to acute stroke, part 1: Drugs, devices, and data
Abstract
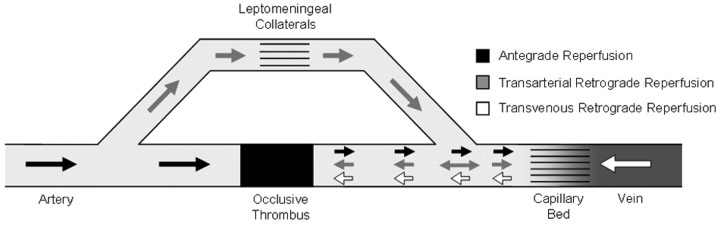
Despite years of research and pioneering clinical work, stroke remains a massive public health concern. Since 1996, we have lived in the era of US Food and Drug Administration-approved intravenous (i.v.) recombinant tissue plasminogen activator (rtPA). This treatment, despite its promise, continues to exhibit its limitations. Endovascular therapy has several theoretic advantages over i.v. rtPA, including site specificity, longer treatment windows, and higher recanalization rates. In this article, we will review the various pharmacologic strategies for acute stroke treatment, providing both a historic context and the state of the art. The drugs will be classified on the basis of their theoretic rationale for therapy. Next, we will review the various devices and strategies for mechanical revascularization with an aim toward comprehensiveness. These range from wire disruption of thrombus to preclinical trials for novel mechanical solutions. This first installment of this 2-part series will end with an analysis of retrograde reperfusion techniques.
Figures

References
-
- Stroke: 1989—recommendations on stroke prevention, diagnosis, and therapy: report of the WHO Task Force on Stroke and other Cerebrovascular Disorders. Stroke 1989;20:1407–31 - PubMed
-
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics: 2008 update—a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2008;117:e25–146 - PubMed
-
- Tissue plasminogen activator for acute ischemic stroke: The National Institute of Neurological Disorders and Stroke rtPA Stroke Study Group. N Engl J Med 1995;333:1581–87 - PubMed
-
- Practice advisory: thrombolytic therapy for acute ischemic stroke—summary statement. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1996;47:835–39 - PubMed
-
- Adams HP Jr, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute ischemic stroke—a statement for healthcare professionals from a Special Writing Group of the Stroke Council. American Heart Association. Circulation 1996;94:1167–74 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical