

Dangerous extracranial-intracranial anastomoses and supply to the cranial nerves: vessels the neurointerventionalist needs to know
- PMID: 19279274
- PMCID: PMC7051597
- DOI: 10.3174/ajnr.A1500
Dangerous extracranial-intracranial anastomoses and supply to the cranial nerves: vessels the neurointerventionalist needs to know
Abstract
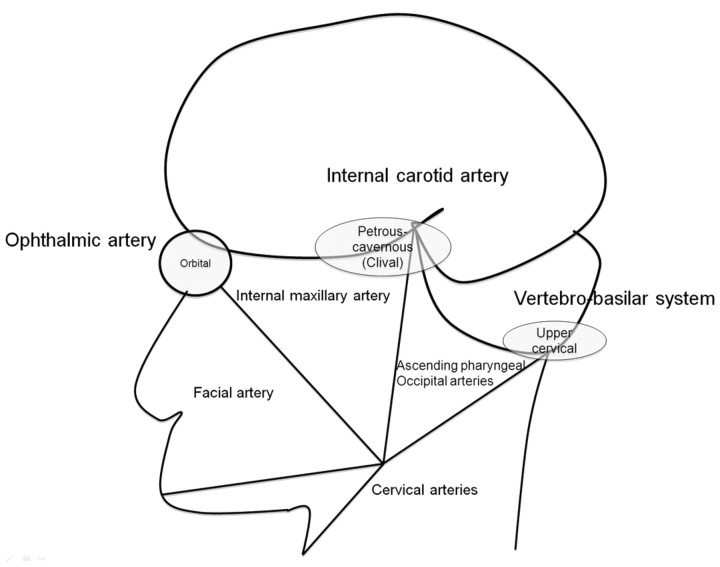
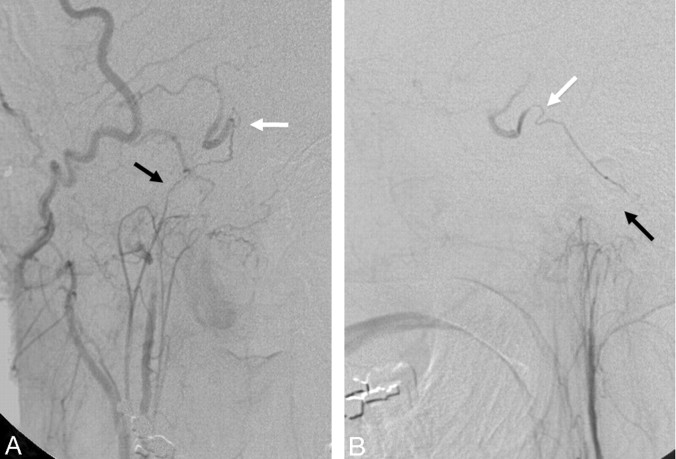
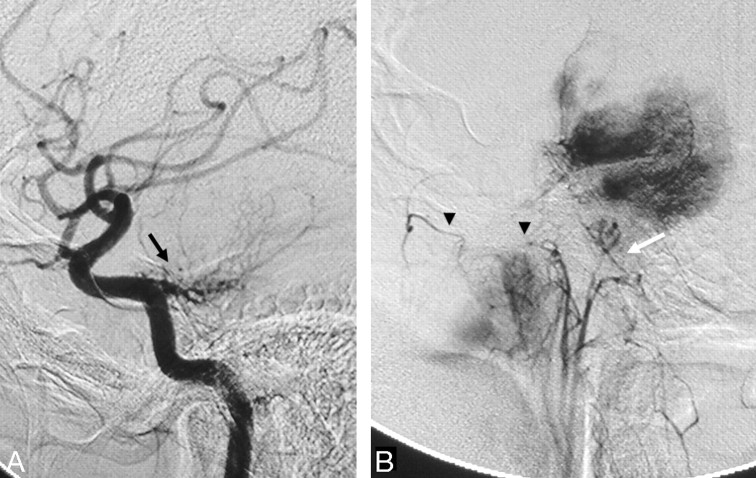
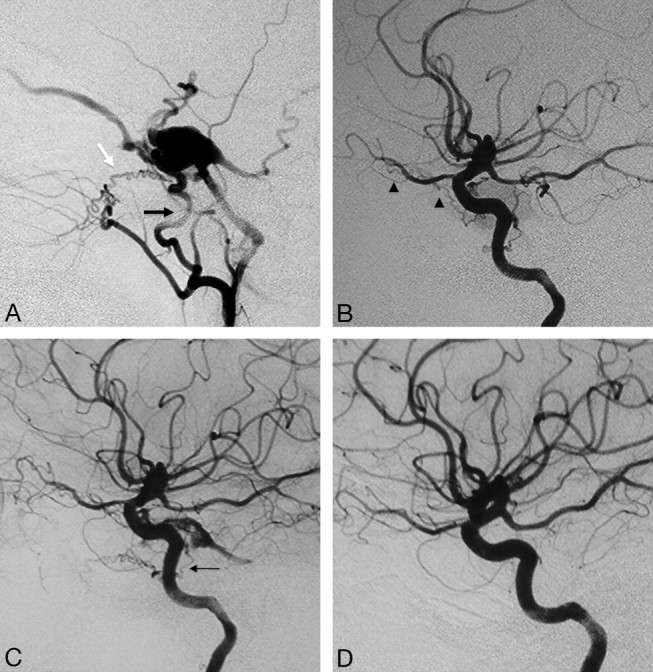
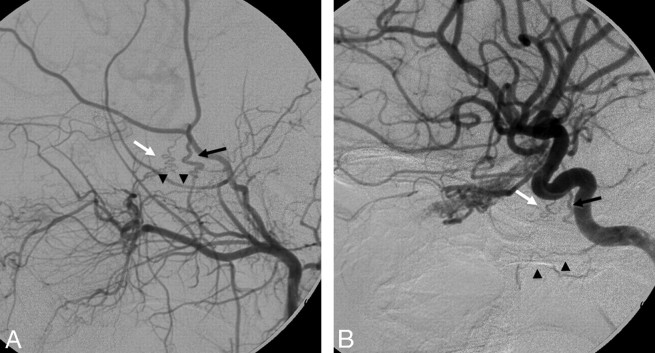
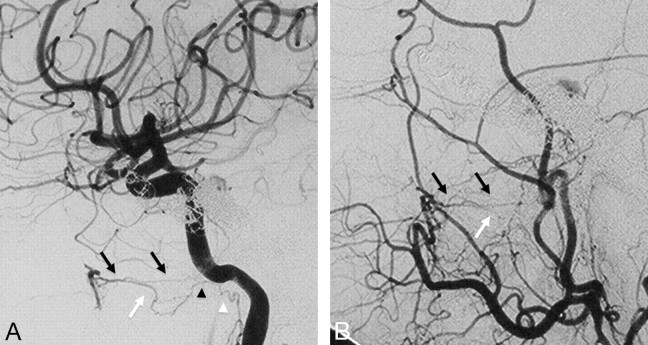
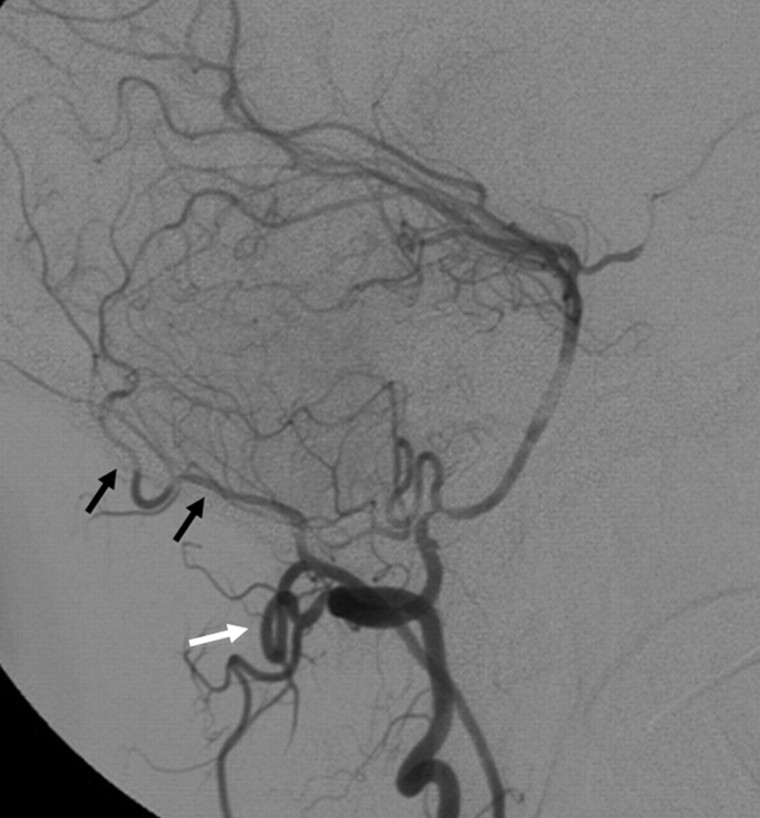
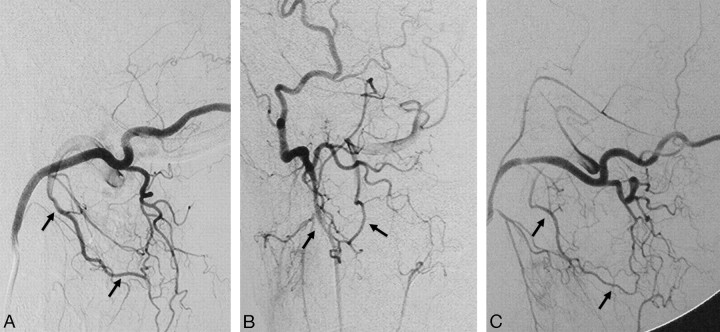
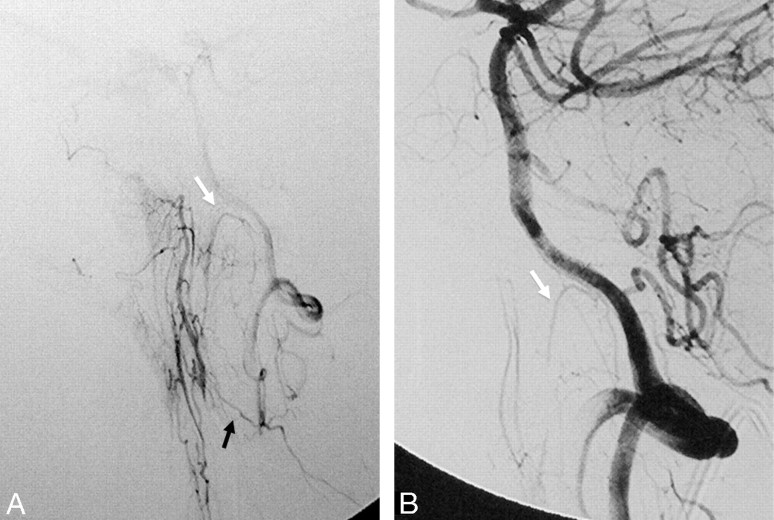
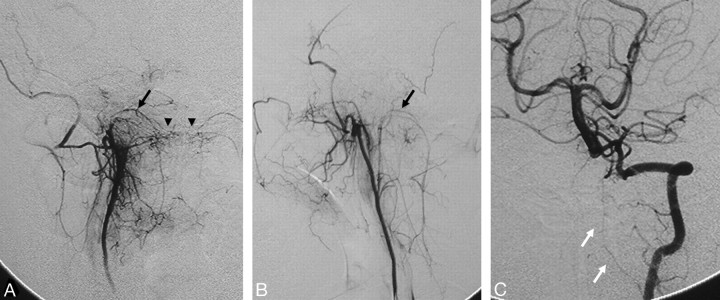
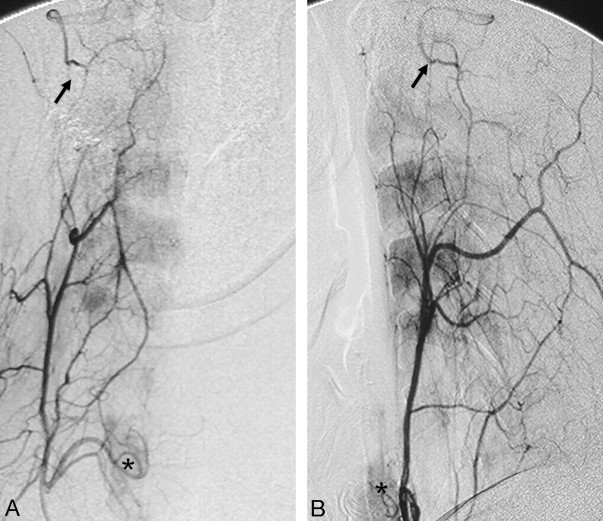
Transarterial embolization in the external carotid artery (ECA) territory has a major role in the endovascular management of epistaxis, skull base tumors, and dural arteriovenous fistulas. Knowledge of the potential anastomotic routes, identification of the cranial nerve supply from the ECA, and the proper choice of embolic material are crucial to help the interventionalist avoid neurologic complications during the procedure. Three regions along the skull base constitute potential anastomotic routes between the extracranial and intracranial arteries: the orbital, the petrocavernous, and the upper cervical regions. Branches of the internal maxillary artery have anastomoses with the ophthalmic artery and petrocavernous internal carotid artery (ICA), whereas the branches of the ascending pharyngeal artery are connected to the petrocavernous ICA. Branches of both the ascending pharyngeal artery and the occipital artery have anastomoses with the vertebral artery. To avoid cranial nerve palsy, one must have knowledge of the supply to the lower cranial nerves: The petrous branch of the middle meningeal artery and the stylomastoid branch of the posterior auricular artery form the facial arcade as the major supply to the facial nerve, and the neuromeningeal trunk of the ascending pharyngeal artery supplies the lower cranial nerves (CN IX-XII).
Figures

References
-
- Agid R, Terbrugge K, Rodesch G, et al. Management strategies for anterior cranial fossa (ethmoidal) dural arteriovenous fistulas with an emphasis on endovascular treatment. J Neurosurg 2009; 110: 79– 84 - PubMed
-
- Shi ZS, Ziegler J, Gonzalez NR, et al. Transarterial embolization of clival dural arteriovenous fistulae using liquid embolic agents. Neurosurgery 2008; 62: 408– 15 - PubMed
-
- Gupta AK, Purkayastha S, Bodhey NK, et al. Preoperative embolization of hypervascular head and neck tumours. Australas Radiol 2007; 51: 446– 52 - PubMed
-
- Kasper GC, Welling RE, Wladis AR, et al. A multidisciplinary approach to carotid paragangliomas. Vasc Endovascular Surg 2006; 40: 467– 74 - PubMed
-
- Persky MS, Setton A, Niimi Y, et al. Combined endovascular and surgical treatment of head and neck paragangliomas: a team approach. Head Neck 2002; 24: 423– 31 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous