

A randomized phase 1 study of testosterone replacement for patients with low-risk castration-resistant prostate cancer
- PMID: 19282098
- PMCID: PMC2885777
- DOI: 10.1016/j.eururo.2009.02.022
A randomized phase 1 study of testosterone replacement for patients with low-risk castration-resistant prostate cancer
Abstract
Background: Even in castration-resistant prostate cancer (CRPC), the androgen pathway remains biologically relevant. In preclinical models, androgen therapy for CRPC leads to growth arrest, apoptosis, and tumor shrinkage.
Objective: This study sought to determine the toxicity and feasibility of a testosterone therapy in early CRPC.
Design, setting, and participants: Prostate cancer patients with progressive disease following androgen ablation, antiandrogen therapy, and withdrawal and no to minimal metastatic disease who were followed at the University of Chicago were randomized to treatment with three doses of transdermal testosterone.
Intervention: Patients were treated with transdermal testosterone at 2.5, 5.0, or 7.5 mg/day.
Measurements: Toxicity, prostate-specific antigen (PSA), imaging, quality of life (QoL), and strength were monitored. Treatment was discontinued for significant toxicity, clinical progression, or a 3-fold increase in PSA.
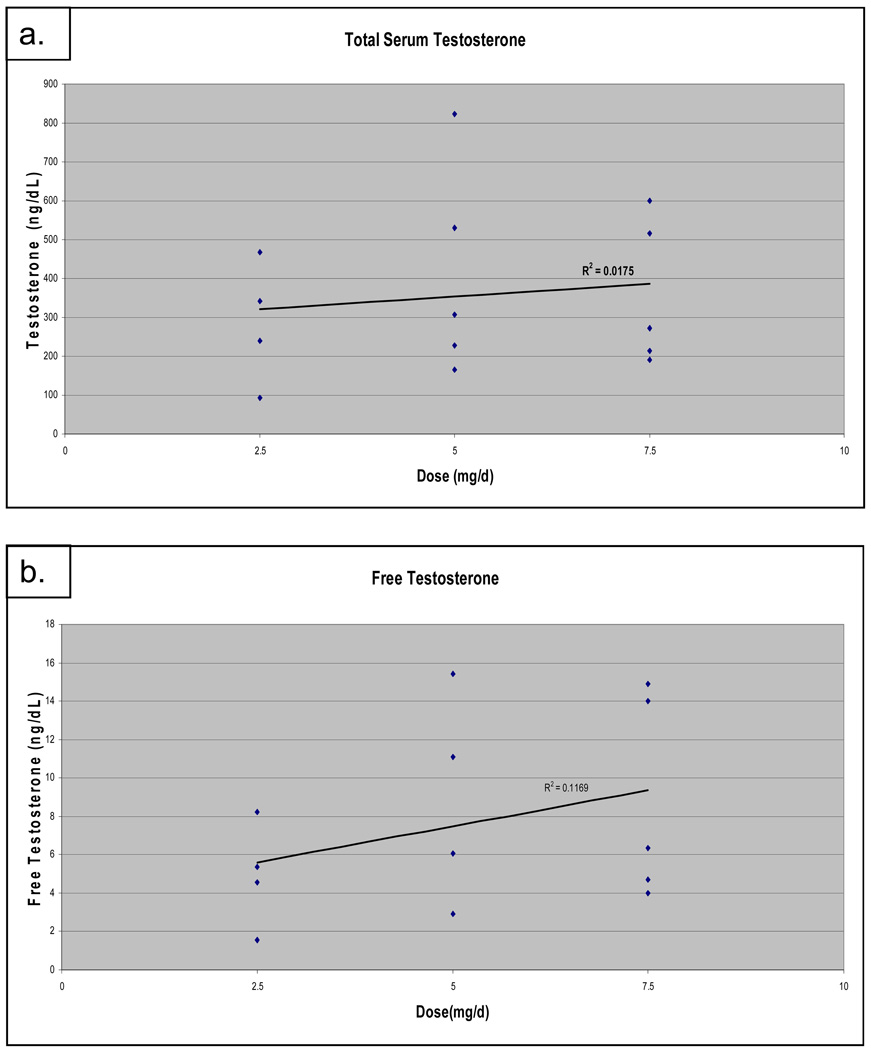
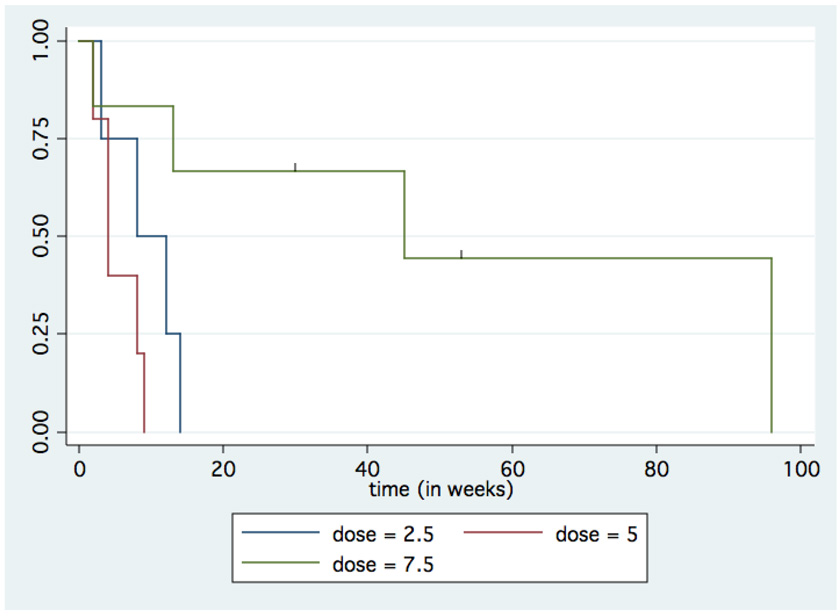
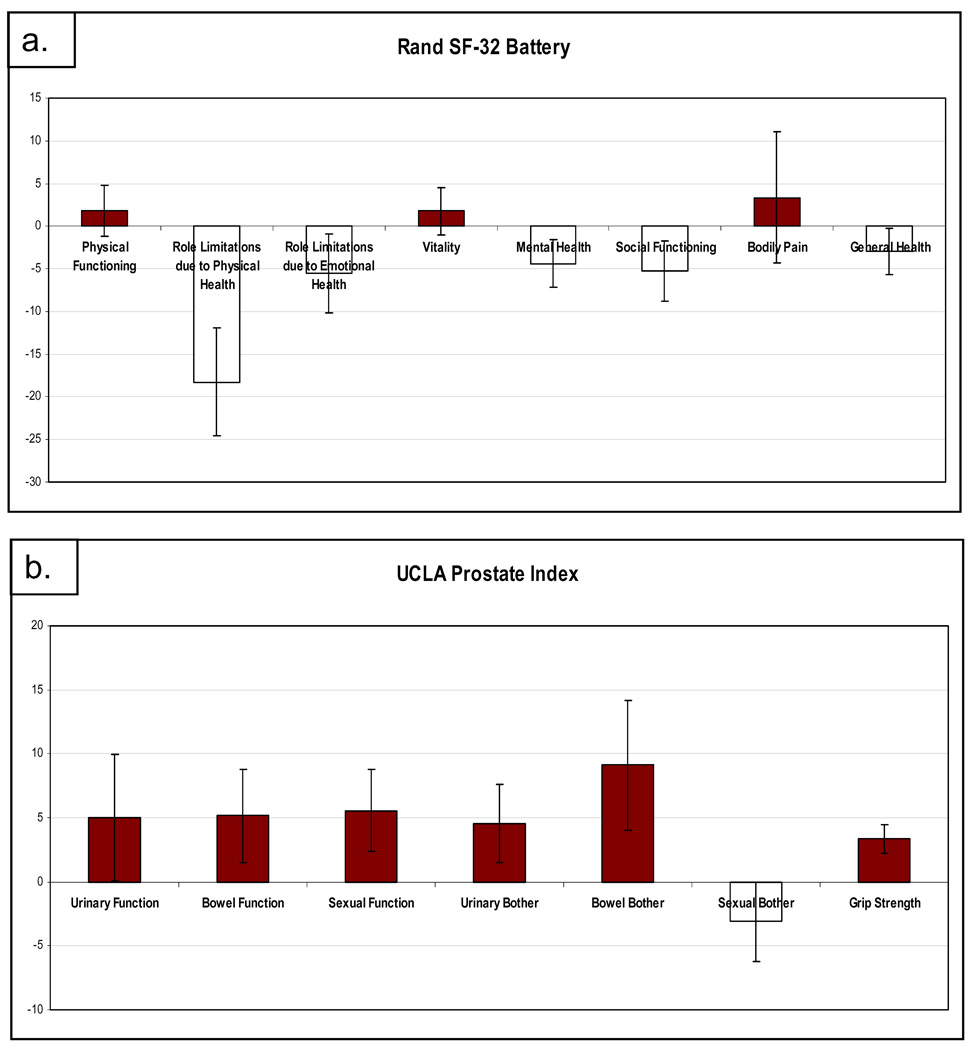
Results and limitations: Fifteen men with a median age of 73 yr (range: 62-92) and a median PSA of 11.1 ng/ml (range: 5.2-63.6) were treated. Testosterone increased from castrate to median concentrations of 305 ng/dl, 308 ng/dl, and 297 ng/dl for dosages of 2.5 mg/day (n=4), 5.0 mg/day (n=5), and 7.5 mg/day (n=5), respectively. One patient was taken off of the study at 53 wk due to grade 4 cardiac toxicity. There were no other grade 3 or 4 toxicities related to the study medication, and the grade 2 toxicities were minimal. Only one patient experienced symptomatic progression, and three (20%) patients demonstrated a decrease in PSA (largest was 43%). Median time to progression was 9 wk (range: 2-96), with no detectable difference in the three dose cohorts. There was no significant improvement in QoL, and there was a borderline statistically significant improvement in hand-grip strength with treatment. The study was limited by sample size, single arm, and variability of baseline patient characteristics.
Conclusions: Testosterone is a feasible and reasonably well-tolerated therapy for men with early CRPC. A larger, randomized trial is under way to further characterize efficacy and impact on QoL measures.
Figures
Comment in
-
Editorial comment on: A randomized phase 1 study of testosterone replacement for patients with low-risk castration-resistant prostate cancer.Eur Urol. 2009 Jul;56(1):103-4. doi: 10.1016/j.eururo.2009.02.023. Epub 2009 Feb 27. Eur Urol. 2009. PMID: 19282103 No abstract available.
-
Re: Russell Szmulewitz, Supriya Mohile, Edwin Posadas, et al. A randomized phase 1 study of testosterone replacement for patients with low-risk castration-resistant prostate cancer. Eur Urol 2009;56:97-104.Eur Urol. 2009 Nov;56(5):e36; author reply e37. doi: 10.1016/j.eururo.2009.07.052. Epub 2009 Aug 12. Eur Urol. 2009. PMID: 19683856 No abstract available.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer Statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Halabi S, Small EJ, Kantoff PW, et al. Prognostic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J Clin Oncol. 2003;21:1232–1237. - PubMed
-
- Smaletz O, Scher HI, Small EJ, et al. Nomogram for overall survival of patients with progressive metastatic prostate cancer after castration. J Clin Oncol. 2002;20:3972–3982. - PubMed
-
- Huggins C, Hodges C. Studies on prostatic cancer. I. The effets of castration, of estrogen, and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Research. 1941;1:293–297.
-
- Huggins C, Stevens RJ, Hodges C. Studies on prostatic cancer. II. The effects of castration on advanced carcinoma of the prostate gland. Archives of Surgery. 1941;43:209–223. Archives of Surgery 43:209–223, 1941.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
