

Classification of scoliosis deformity three-dimensional spinal shape by cluster analysis
- PMID: 19282737
- PMCID: PMC2664249
- DOI: 10.1097/BRS.0b013e318190b914
Classification of scoliosis deformity three-dimensional spinal shape by cluster analysis
Abstract
Study design: Cluster analysis of existing database of spinal shape of patients attending a scoliosis clinic.
Objective: To determine whether patients with scoliosis can be classified into distinct groups by 3-dimensional curve shape.
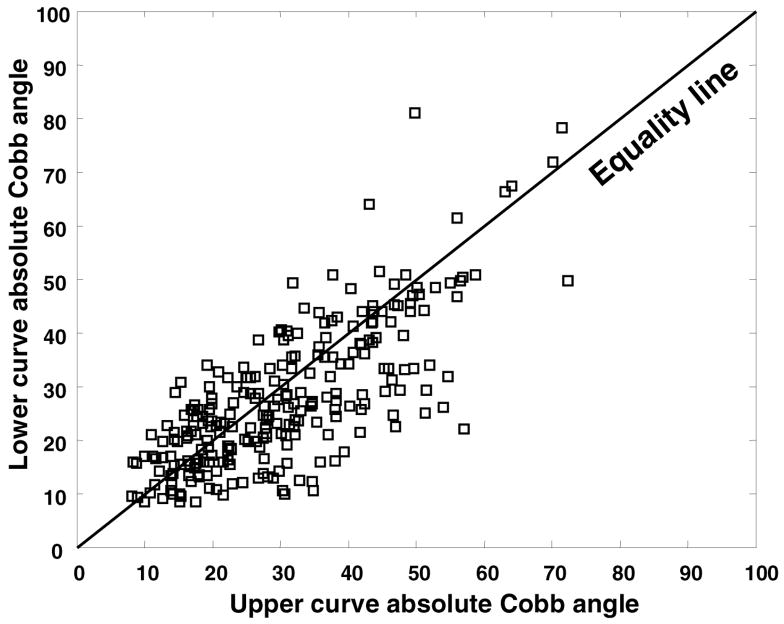
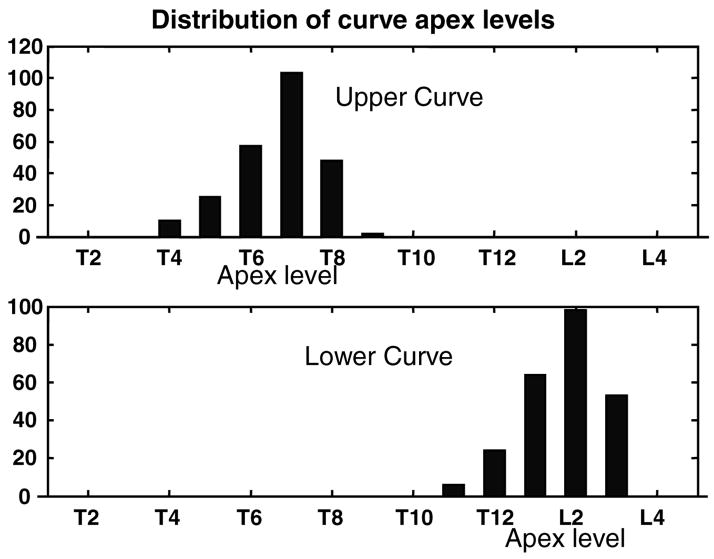
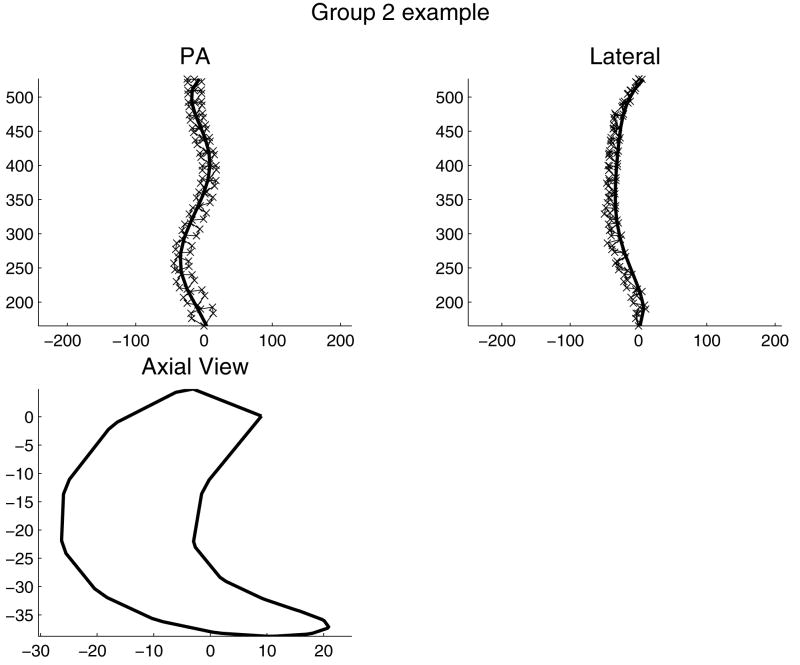
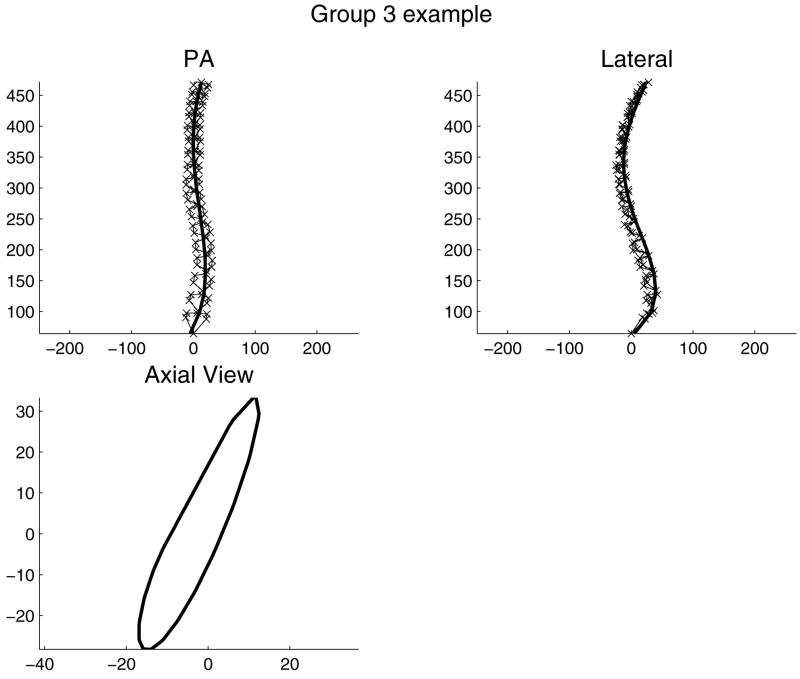
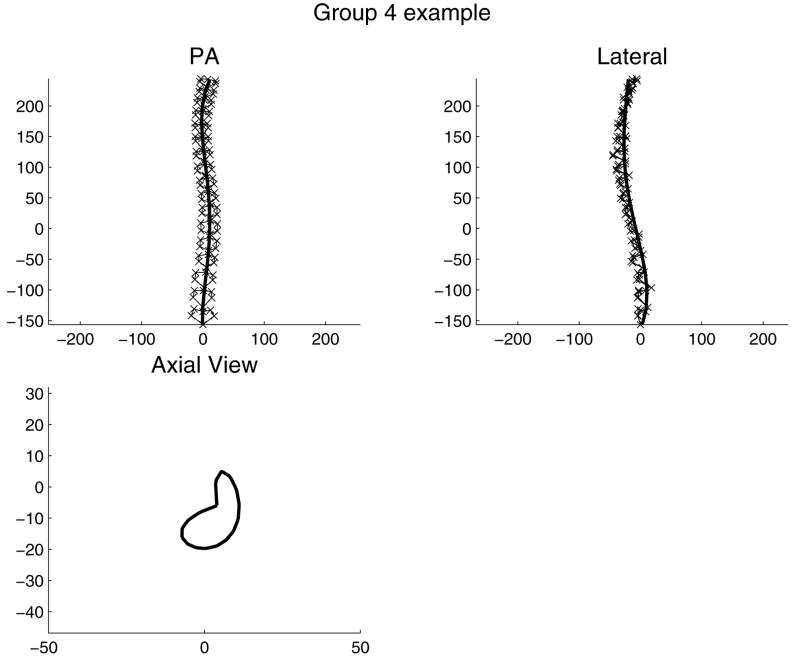
Summary of background data: Subjective or semiquantitative methods can be used to classify curve types in scoliosis, with the goal of rationalizing surgical planning. There are very few reports of using objective methods such as cluster analysis to improve this process. METHODS.: One hundred ten patients who underwent radiography of the spine by a stereo technique, at a scoliosis clinic in the period between 1982 and 1990, were studied. Fifty-six were studied longitudinally (average 3.4 clinic visits each), providing 245 total observations. Selected patients had 2 scoliosis curves with apex between T4 and L3, and both Cobb angles >9 degrees by an automated measurement. The 3-dimensional spinal shape was reconstructed from stereoradiographs. Each curve was quantified by its Cobb angle, apex level, apex vertebra rotation, and rotation of the plane of maximum curvature (PMC) (8 variables). Cluster analysis classified each patient at each visit by these variables.
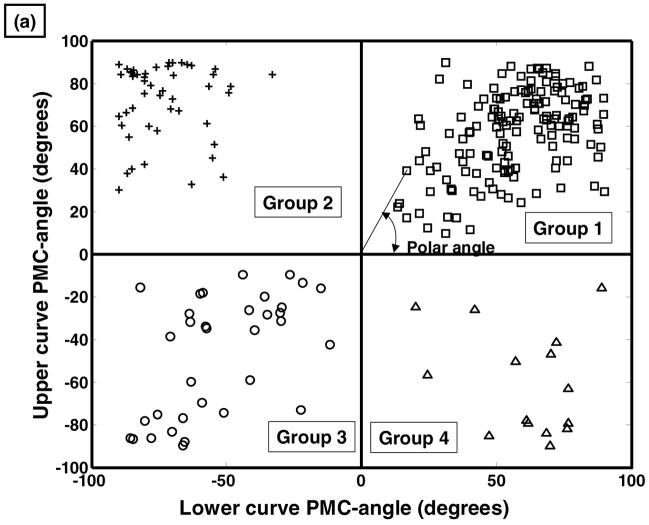
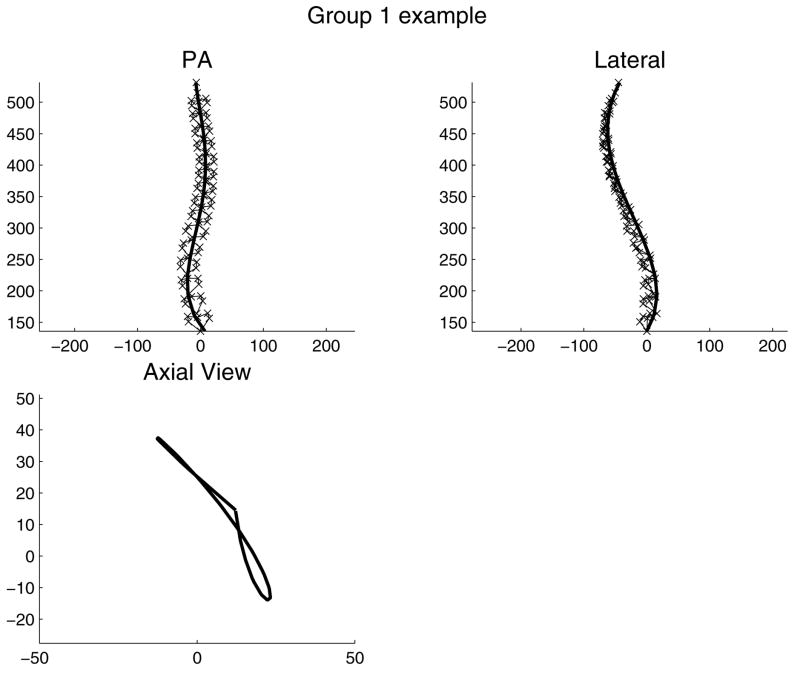
Results: When the analysis searched for 4 clusters, the largest cluster (148 of 245 observations) was the pattern having counterclockwise rotation of the PMC of both curves (typically, a right upper scoliosis curve with kyphosis and left lower scoliosis curve with lordosis). The other 3 clusters (48, 34, and 15 observations) were the other permutations of these variables. Substantial overlap of all the other variables between groups was observed. Of the 56 patients seen longitudinally, 25 were consistently grouped at all clinic visits.
Conclusion: Spinal shape of patients in a clinic population with 2 scoliosis curves form distinct groups according to the 4 permutations of the signs of the rotations of the PMC in 2 curve regions. The pattern can change with repeated observation, often because a slight curvature in the sagittal plane can change because of postural variation and measurement errors. Overlap of the other curve-shape variables between groups suggests that these spinal deformity classifications alone should not determine treatment strategy.
Figures


References
-
- King HA, Moe JH, Bradford DS, Winter RB. The selection of fusion levels in thoracic idiopathic scoliosis. J Bone Joint Surg. 1983;65:1302–1313. - PubMed
-
- Lenke LG, Betz RR, Harms J, et al. Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. J Bone Joint Surg Am. 2001;83:1169–81. - PubMed
-
- Stokes IA, Aronsson DD. Computer-assisted algorithms improve reliability of King classification and Cobb angle measurement of scoliosis. Spine. 2006;31(6):665–670. - PubMed
-
- Duong L, Chariet F, Labelle H. Three-dimensional classification of spinal deformities using fuzzy clustering. Spine. 2006;31(8):923–930. - PubMed
-
- Stokes IAF, Bigalow LC, Moreland MS. Three-dimensional spinal curvature in idiopathic scoliosis. J Orthop Res. 1987;5:102–113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
