

Coronary arterial calcification in rheumatoid arthritis: comparison with the Multi-Ethnic Study of Atherosclerosis
- PMID: 19284547
- PMCID: PMC2688181
- DOI: 10.1186/ar2641
Coronary arterial calcification in rheumatoid arthritis: comparison with the Multi-Ethnic Study of Atherosclerosis
Abstract
Introduction: Although cardiovascular morbidity and mortality are increased in rheumatoid arthritis, little is known about the burden of subclinical coronary atherosclerosis in these patients.
Methods: Using computed tomography, coronary artery calcification was measured in 195 men and women with rheumatoid arthritis aged 45 to 84 years without clinical cardiovascular disease and compared with 1,073 controls without rheumatoid arthritis enrolled in the Baltimore cohort of the Multi-Ethnic Study of Atherosclerosis.
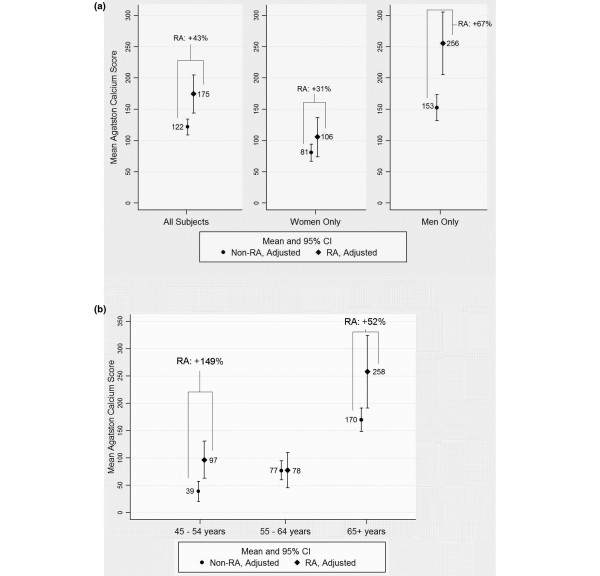
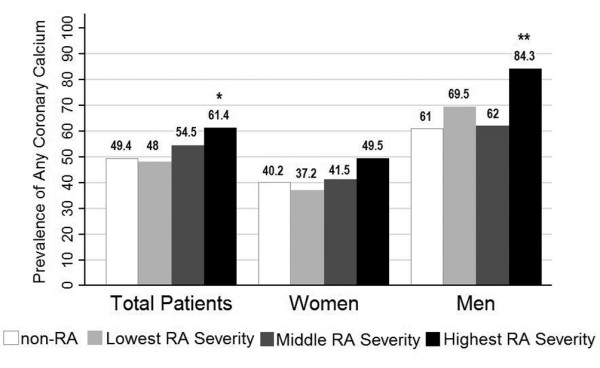
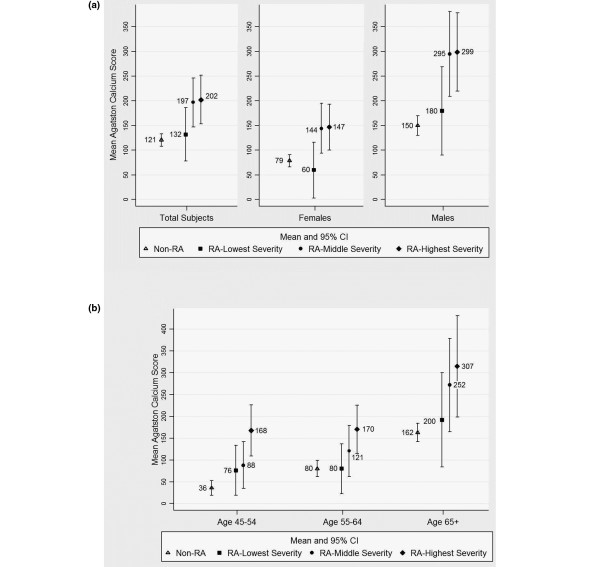
Results: The prevalence of coronary calcification (Agatston score > 0) was significantly higher in men, but not women, with rheumatoid arthritis after adjusting for sociodemographic and cardiovascular risk factors (prevalence ratio = 1.19; P = 0.012). Among participants with prevalent calcification, those with rheumatoid arthritis had adjusted mean Agatston scores 53 units higher than controls (P = 0.002); a difference greater for men than women (P for interaction = 0.017). In all analyses, serum IL-6 attenuated the association between rheumatoid arthritis and coronary calcification, suggesting its role as a potential mediator of enhanced atherosclerosis. Notably, increasing severity of rheumatoid arthritis was associated with a higher prevalence and extent of coronary calcification among both men and women with rheumatoid arthritis, and for all age categories. The largest percentage difference in coronary arterial calcification between rheumatoid arthritis patients and their nonrheumatoid arthritis counterparts was observed in the youngest age category.
Conclusions: Increasing rheumatoid arthritis disease severity was associated with a higher prevalence and greater extent of coronary artery calcification, potentially mediated through an atherogenic effect of chronic systemic inflammation. Gender and age differences in association with coronary calcification suggest that preventive measures should be emphasized in men with rheumatoid arthritis, and considered even in younger rheumatoid arthritis patients with low levels of traditional cardiovascular risk factors.
Figures
References
-
- Wolfe F, Freundlich B, Straus WL. Increase in cardiovascular and cerebrovascular disease prevalence in rheumatoid arthritis. J Rheumatol. 2003;30:36–40. - PubMed
-
- Gonzalez-Juanatey C, Llorca J, Testa A, Revuelta J, Garcia-Porrua C, Gonzalez-Gay MA. Increased prevalence of severe subclinical atherosclerotic findings in long-term treated rheumatoid arthritis patients without clinically evident atherosclerotic disease. Medicine (Baltimore) 2003;82:407–413. doi: 10.1097/01.md.0000101572.76273.60. - DOI - PubMed
-
- Roman MJ, Moeller E, Davis A, Paget SA, Crow MK, Lockshin MD, Sammaritano L, Devereux RB, Schwartz JE, Levine DM, Salmon JE. Preclinical carotid atherosclerosis in patients with rheumatoid arthritis. Ann Intern Med. 2006;144:249–256. - PubMed
-
- Chung CP, Oeser A, Raggi P, Gebretsadik T, Shintani AK, Sokka T, Pincus T, Avalos I, Stein CM. Increased coronary-artery atherosclerosis in rheumatoid arthritis: relationship to disease duration and cardiovascular risk factors. Arthritis Rheum. 2005;52:3045–3053. doi: 10.1002/art.21288. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
