

Refeeding syndrome--awareness, prevention and management
- PMID: 19284691
- PMCID: PMC2654033
- DOI: 10.1186/1758-3284-1-4
Refeeding syndrome--awareness, prevention and management
Abstract
Background: Refeeding syndrome is an important, yet commonly overlooked condition affecting patients. It occurs when feeding is commenced after a period of starvation. Head and neck cancer patients are at particular risk owing to prolonged periods of poor nutritional intake. This may be from general effects such as cancer anorexia or from more specific problems of dysphagia associated with this group of patients. Awareness of the condition is crucial in identifying patients at risk and taking measures to prevent its occurrence.
Objectives: The aims of this review are to: 1) Highlight the condition and stress the importance of its consideration when admitting head and neck cancer patients. 2) Discuss the pathophysiology behind refeeding syndrome. 3) Review the literature for the best available evidence and guidelines. 4) Highlight the need for further high quality research.
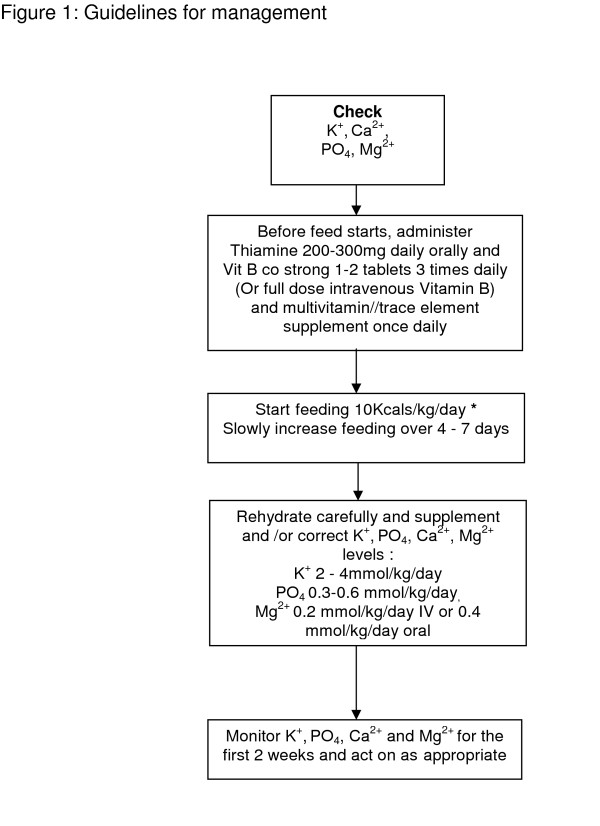
Conclusion: Refeeding syndrome is potentially fatal, yet is preventable. Awareness and identification of at-risk patients is crucial to improving management. Refeeding syndrome is caused by rapid refeeding after a period of under-nutrition, characterised by hypophosphataemia, electrolyte shifts and has metabolic and clinical complications. High risk patients include the chronically under-nourished and those with little intake for greater than 10 days. Patients with dysphagia are at particular risk. Refeeding should commence at 10 kcal/kg per day in patients at risk, and increased slowly. Thiamine, vitamin B complex and multi-vitamin supplements should be started with refeeding. New NICE guidelines state that pre-feeding correction of electrolyte and fluid deficits is unnecessary, but should be done concurrently with re-feeding. More research in this field is needed as the evidence base is lacking.
Figures
References
-
- Schnitker MA, Mattman PE, Bliss TL. A clinical study of malnutrition in Japanese prisoners of war. Ann Intern Med. 1951;35:69–96. - PubMed
-
- Camp MA, Allon M. Severe hypophosphatemia in hospitalised patients. Mineral & Electrolyte Metabolism. pp. 365–368. - PubMed
-
- Marik PE, Bedigan MK. Refeeding Hypophosphataemia in an Intensive Care Unit: A Prospective Study. Arch Surg. 131:1043–1047. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
