

Haplotype-sharing analysis implicates chromosome 7q36 harboring DPP6 in familial idiopathic ventricular fibrillation
- PMID: 19285295
- PMCID: PMC2667995
- DOI: 10.1016/j.ajhg.2009.02.009
Haplotype-sharing analysis implicates chromosome 7q36 harboring DPP6 in familial idiopathic ventricular fibrillation
Abstract
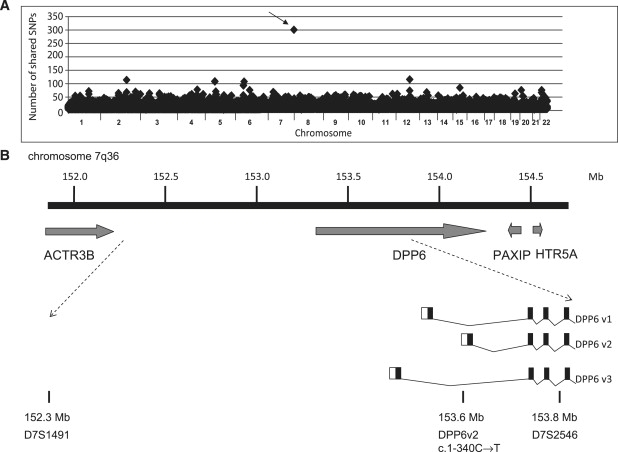
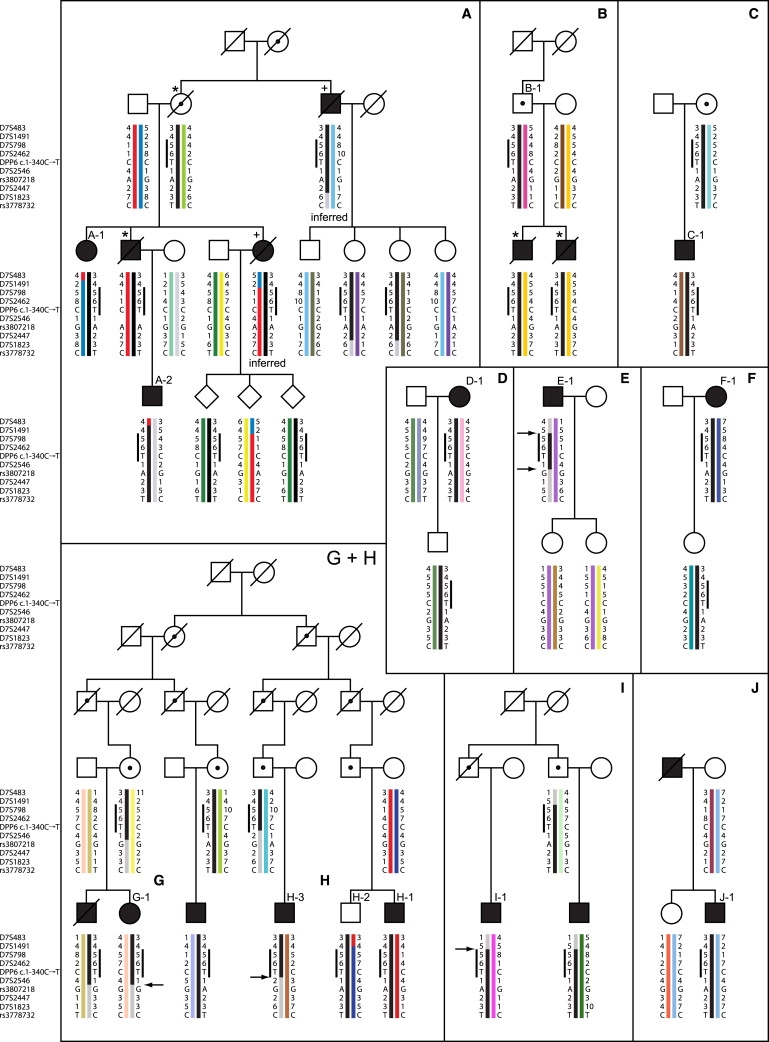
Idiopathic Ventricular Fibrillation (IVF) is defined as spontaneous VF without any known structural or electrical heart disease. A family history is present in up to 20% of probands with the disorder, suggesting that at least a subset of IVF is hereditary. A genome-wide haplotype-sharing analysis was performed for identification of the responsible gene in three distantly related families in which multiple individuals died suddenly or were successfully resuscitated at young age. We identified a haplotype, on chromosome 7q36, that was conserved in these three families and was also shared by 7 of 42 independent IVF patients. The shared chromosomal segment harbors part of the DPP6 gene, which encodes a putative component of the transient outward current in the heart. We demonstrated a 20-fold increase in DPP6 mRNA levels in the myocardium of carriers as compared to controls. Clinical evaluation of 84 risk-haplotype carriers and 71 noncarriers revealed no ECG or structural parameters indicative of cardiac disease. Penetrance of IVF was high; 50% of risk-haplotype carriers experienced (aborted) sudden cardiac death before the age of 58 years. We propose DPP6 as a gene for IVF and increased DPP6 expression as the likely pathogenetic mechanism.
Figures



References
-
- Zipes D.P., Camm A.J., Borggrefe M., Buxton A.E., Chaitman B., Fromer M., Gregoratos G., Klein G., Moss A.J., Myerburg R.J. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e385–e484. - PubMed
-
- Consensus Statement of the Joint Steering Committees of the Unexplained Cardiac Arrest Registry of Europe and of the Idiopathic Ventricular Fibrillation Registry of the United States Survivors of out-of-hospital cardiac arrest with apparently normal heart. Need for definition and standardized clinical evaluation. Circulation. 1997;95:265–272. - PubMed
-
- Zipes D.P., Wellens H.J. Sudden cardiac death. Circulation. 1998;98:2334–2351. - PubMed
-
- Haissaguerre M., Shoda M., Jaïs P., Nogami A., Shah D.C., Kautzner J., Arentz T., Kalushe D., Lamaison D., Griffith M. Mapping and ablation of idiopathic ventricular fibrillation. Circulation. 2002;106:962–967. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
