

Percutaneous coronary interventions for non-acute coronary artery disease: a quantitative 20-year synopsis and a network meta-analysis
- PMID: 19286090
- PMCID: PMC2967219
- DOI: 10.1016/S0140-6736(09)60319-6
Percutaneous coronary interventions for non-acute coronary artery disease: a quantitative 20-year synopsis and a network meta-analysis
Erratum in
- Lancet. 2009 Aug 1;374(9687):378
Abstract
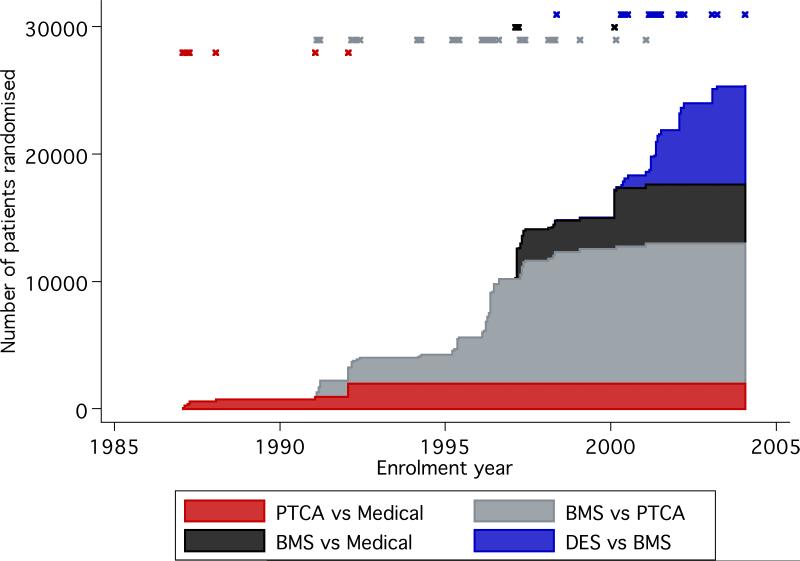
Background: Over the past 20 years, percutaneous transluminal balloon coronary angioplasty (PTCA), bare-metal stents (BMS), and drug-eluting stents (DES) succeeded each other as catheter-based treatments for coronary artery disease. We undertook a systematic overview of randomised trials comparing these interventions with each other and with medical therapy in patients with non-acute coronary artery disease.
Methods: We searched Medline for trials contrasting at least two of the four interventions (PTCA, BMS, DES, and medical therapy). Eligible outcomes were death, myocardial infarction, coronary artery bypass grafting, target lesion or vessel revascularisation, and any revascularisation. Random effects meta-analyses summarised head-to-head (direct) comparisons, and network meta-analyses integrated direct and indirect evidence.
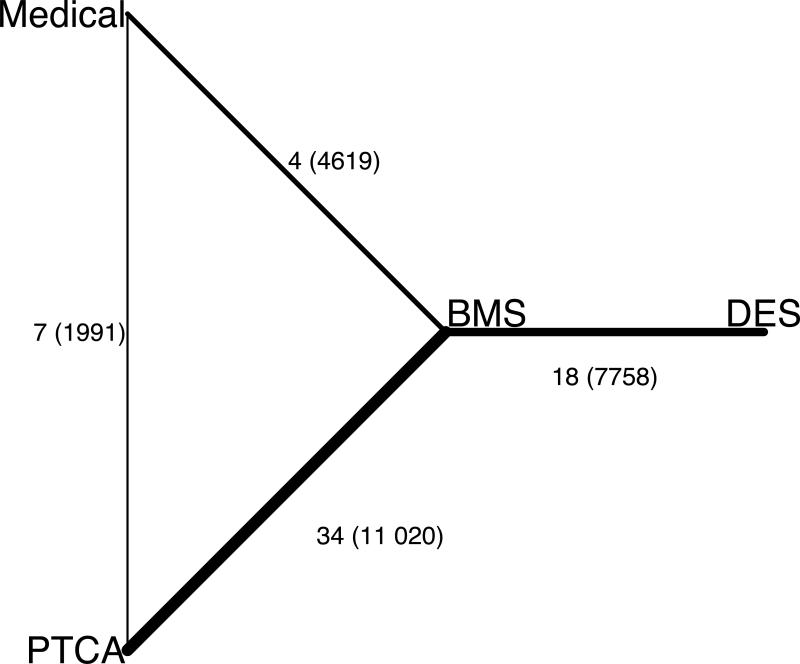
Findings: 61 eligible trials (25 388 patients) investigated four of six possible comparisons between the four interventions; no trials directly compared DES with medical therapy or PTCA. In all direct or indirect comparisons, succeeding advancements in percutaneous coronary intervention did not produce detectable improvements in deaths or myocardial infarction. The risk ratio (RR) for indirect comparisons between DES and medical therapy was 0.96 (95% CI 0.60-1.52) for death and 1.15 (0.73-1.82) for myocardial infarction. By contrast, we recorded sequential significant reductions in target lesion or vessel revascularisation with BMS compared with PTCA (RR 0.68 [0-60.0.77]) and with DES compared with BMS (0.44 [0.35-0.56]). The RR for the indirect comparison between DES and PTCA for target lesion or vessel revascularisation was 0.30 (0.17-0.51).
Interpretation: Sequential innovations in the catheter-based treatment of non-acute coronary artery disease showed no evidence of an effect on death or myocardial infarction when compared with medical therapy. These results lend support to present recommendations to optimise medical therapy as an initial management strategy in patients with this disease.
Figures
Comment in
-
Effectiveness of PCI for non-acute coronary artery disease.Lancet. 2009 Mar 14;373(9667):870-2. doi: 10.1016/S0140-6736(09)60522-5. Lancet. 2009. PMID: 19286067 No abstract available.
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, et al. Heart disease and stroke statistics--2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–146. - PubMed
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Mehta SR, Cannon CP, Fox KA, Wallentin L, Boden WE, Spacek R, et al. Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of randomized trials. JAMA. 2005;293:2908–17. - PubMed
-
- Brophy JM, Belisle P, Joseph L. Evidence for use of coronary stents. A hierarchical bayesian meta-analysis. Ann Intern Med. 2003;138:777–86. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
