

Metabolic complications of androgen deprivation therapy for prostate cancer
- PMID: 19286225
- PMCID: PMC2900631
- DOI: 10.1016/j.juro.2009.01.047
Metabolic complications of androgen deprivation therapy for prostate cancer
Abstract
Purpose: Androgen deprivation therapy has a variety of well recognized adverse effects including vasomotor flushing, loss of libido, fatigue, gynecomastia, anemia and osteoporosis. This review focuses on the more recently described metabolic complications of androgen deprivation therapy including obesity, insulin resistance and lipid alterations as well as the association of androgen deprivation therapy with diabetes and cardiovascular disease.
Materials and methods: We reviewed the medical literature using the PubMed(R) search terms prostate cancer, androgen deprivation therapy, gonadotropin-releasing hormone agonists, obesity, insulin resistance, lipids, diabetes, cardiovascular disease and myocardial infarction. We provide a focused review and our perspective on the relevant literature.
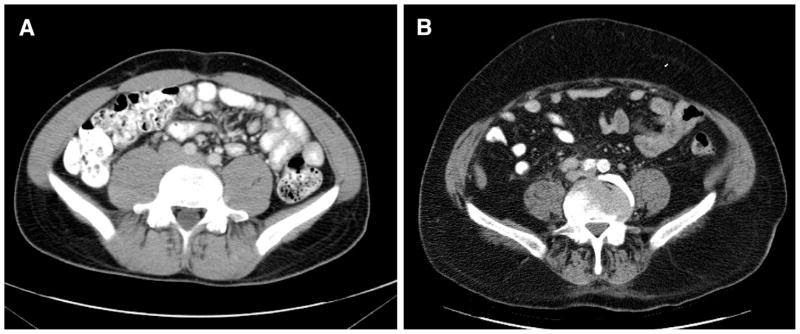
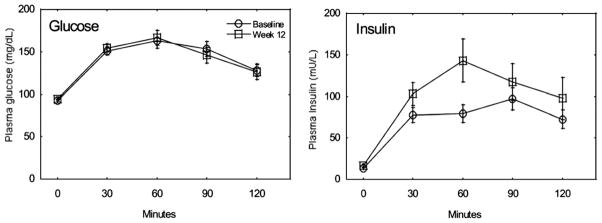
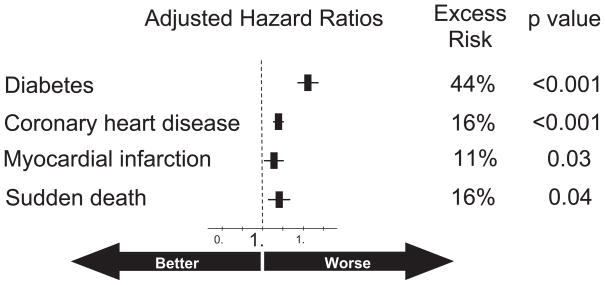
Results: Androgen deprivation therapy decreases lean mass and increases fat mass. It also decreases insulin sensitivity while increasing low density lipoprotein cholesterol, high density lipoprotein cholesterol and triglycerides. Consistent with these adverse metabolic effects, androgen deprivation therapy may be associated with a greater incidence of diabetes and cardiovascular disease. Some of these androgen deprivation therapy related metabolic changes (obesity, insulin resistance and increased triglycerides) overlap with features of the metabolic syndrome. However, in contrast to the metabolic syndrome, androgen deprivation therapy increases subcutaneous fat and high density lipoprotein cholesterol.
Conclusions: Androgen deprivation therapy increases obesity, decreases insulin sensitivity and adversely alters lipid profiles. It may be associated with a greater incidence of diabetes and cardiovascular disease. The benefits of androgen deprivation therapy should be weighed against these and other potential harms. Little is known about the optimal strategy to mitigate the adverse metabolic effects of androgen deprivation therapy. Thus, we recommend an emphasis on existing strategies for screening and treatment that have been documented to reduce the risk of diabetes and cardiovascular disease in the general population.
Figures
References
-
- SEER. Surveillance, Epidemiology and End Results (SEER): Stat Fact Sheets: Prostate Cancer. 2008.
-
- Bolla M, Gonzalez D, Warde P, Dubois JB, Mirimanoff RO, Storme G, et al. Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N Engl J Med. 1997;337:295. - PubMed
-
- D’Amico AV, Manola J, Loffredo M, Renshaw AA, DellaCroce A, Kantoff PW. 6-Month androgen suppression plus radiation therapy vs radiation therapy alone for patients with clinically localized prostate cancer: a randomized controlled trial. JAMA. 2004;292:821. - PubMed
-
- Walsh PC. Immediate versus deferred treatment for advanced prostatic cancer: initial results of the Medical Research Council trial. The Medical Research Council Prostate Cancer Working Party Investigators Group. J Urol. 1997;158:1623. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
