

Autosomal dominant C1149R von Willebrand disease: phenotypic findings and their implications
- PMID: 19286880
- PMCID: PMC2675680
- DOI: 10.3324/haematol.2008.003301
Autosomal dominant C1149R von Willebrand disease: phenotypic findings and their implications
Abstract
Background: Mutation C1149R in the von Willebrand factor (VWF) gene has been thought to cause autosomal dominant severe type 1 von Willebrand disease (VWD).
Design and methods: Eight patients from three unrelated families with this mutation were included in the present study who had distinct VWF abnormalities, not described in earlier studies.
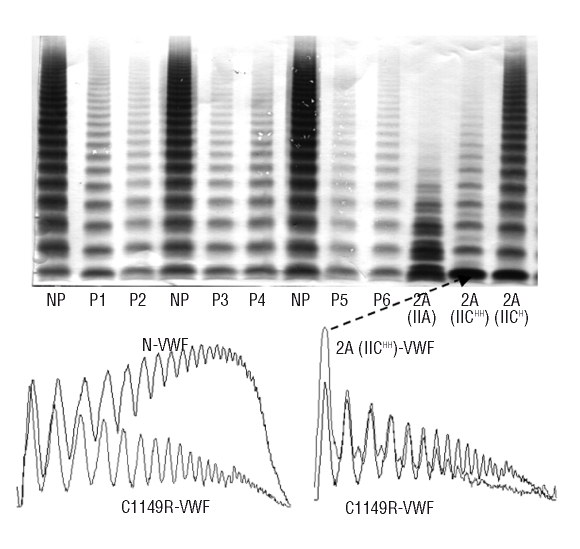
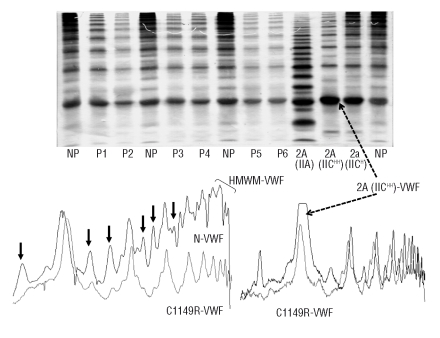
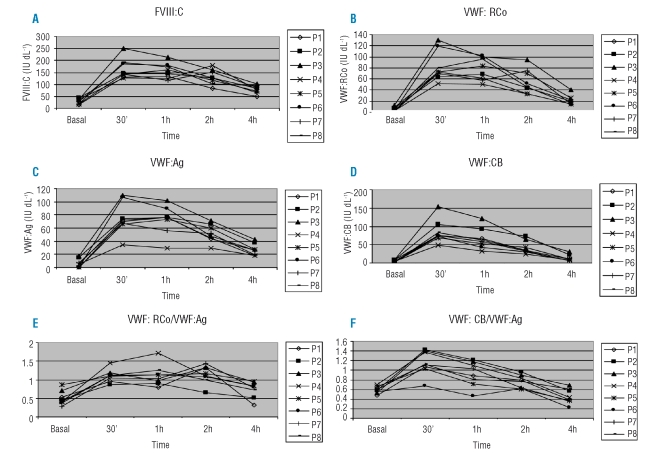
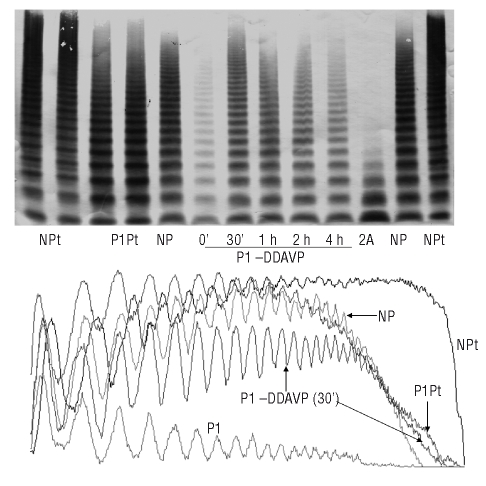
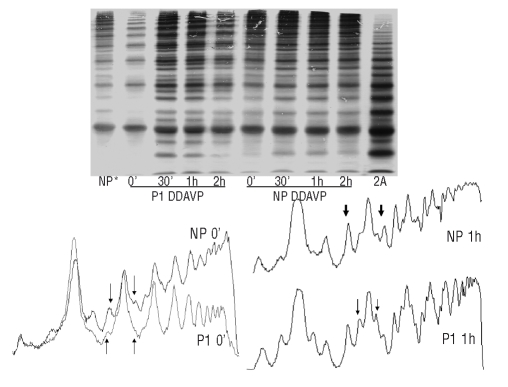
Results: The patients showed notably low levels of VWF antigen (VWF:Ag), VWF ristocetin cofactor activity (VWF:RCo), VWF collagen binding (VWF:CB), and a reduced ristocetin-induced platelet aggregation (RIPA). VWF:RCo/VWF:Ag and VWF:CB/VWF:Ag ratios were lower than 0.7. At basal conditions, all the VWF multimers were decreased in plasma, with a clearly lower relative proportion of the high molecular weight VWF multimers (HMWM). In high-resolution agarose gels, a large decrease in the relative proportions of the satellite bands was seen. The patients had a brief good response to desmopressin (DDAVP) administration, but the released VWF half-life was shorter than normal, indicating an accelerated clearance of their VWF. Platelet VWF was abnormal.
Conclusions: We conclude from the results obtained in these patients for plasma phenotypic data that this mutation should be classified as a VWD type 2A (IIE). DDAVP therapy may be somewhat helpful for this mutation, at least for mild to moderate bleeding. These data provide evidence that for VWD classification factors other than basal VWF, such as DDAVP response and platelet VWF, should be considered.
Figures
Comment in
-
Clinical and laboratory versus molecular markers for a correct classification of von Willebrand disease.Haematologica. 2009 May;94(5):610-5. doi: 10.3324/haematol.2009.005751. Haematologica. 2009. PMID: 19407316 Free PMC article.
Similar articles
-
Laboratory diagnosis of von Willebrand disease type 1/2E (2A subtype IIE), type 1 Vicenza and mild type 1 caused by mutations in the D3, D4, B1-B3 and C1-C2 domains of the von Willebrand factor gene. Role of von Willebrand factor multimers and the von Willebrand factor propeptide/antigen ratio.Acta Haematol. 2009;121(2-3):128-38. doi: 10.1159/000214853. Epub 2009 Jun 8. Acta Haematol. 2009. PMID: 19506359 Review.
-
Laboratory diagnosis and molecular classification of von Willebrand disease.Acta Haematol. 2009;121(2-3):71-84. doi: 10.1159/000214846. Epub 2009 Jun 8. Acta Haematol. 2009. PMID: 19506352 Review.
-
Dominant von Willebrand disease type 2M and 2U are variable expressions of one distinct disease entity caused by loss-of-function mutations in the A1 domain of the von Willebrand factor gene.Acta Haematol. 2009;121(2-3):145-53. doi: 10.1159/000214855. Epub 2009 Jun 8. Acta Haematol. 2009. PMID: 19506361 Review.
-
Characterization, classification, and treatment of von Willebrand diseases: a critical appraisal of the literature and personal experiences.Semin Thromb Hemost. 2005 Nov;31(5):577-601. doi: 10.1055/s-2005-922230. Semin Thromb Hemost. 2005. PMID: 16276467 Review.
-
Dominant von Willebrand disease type 2A groups I and II due to missense mutations in the A2 domain of the von Willebrand factor gene: diagnosis and management.Acta Haematol. 2009;121(2-3):154-66. doi: 10.1159/000214856. Epub 2009 Jun 8. Acta Haematol. 2009. PMID: 19506362 Review.
Cited by
-
Identification of von Willebrand factor D4 domain mutations in patients of Afro-Caribbean descent: In vitro characterization.Res Pract Thromb Haemost. 2022 Jun 15;6(4):e12737. doi: 10.1002/rth2.12737. eCollection 2022 May. Res Pract Thromb Haemost. 2022. PMID: 35734101 Free PMC article.
-
von Willebrand's disease diagnosis and laboratory issues.Haemophilia. 2010 Jul;16 Suppl 5(0 5):67-73. doi: 10.1111/j.1365-2516.2010.02296.x. Haemophilia. 2010. PMID: 20590859 Free PMC article. Review.
-
Role of multimeric analysis of von Willebrand factor (VWF) in von Willebrand disease (VWD) diagnosis: Lessons from the PCM-EVW-ES Spanish project.PLoS One. 2018 Jun 20;13(6):e0197876. doi: 10.1371/journal.pone.0197876. eCollection 2018. PLoS One. 2018. PMID: 29924855 Free PMC article.
-
Identification and functional analysis of a novel von Willebrand factor mutation in a family with type 2A von Willebrand disease.PLoS One. 2012;7(3):e33263. doi: 10.1371/journal.pone.0033263. Epub 2012 Mar 27. PLoS One. 2012. PMID: 22479377 Free PMC article.
-
Clinical and laboratory versus molecular markers for a correct classification of von Willebrand disease.Haematologica. 2009 May;94(5):610-5. doi: 10.3324/haematol.2009.005751. Haematologica. 2009. PMID: 19407316 Free PMC article.
References
-
- Sadler JE. Biochemistry and genetics of von Willebrand factor. Annu Rev Biochem. 1998;67:395–424. - PubMed
-
- Sadler JE, Budde U, Eikenboom JC, Favaloro EJ, Hill FG, Holmberg L, et al. Update on the pathophysiology and classification of von Willebrand disease: a report of the Subcommittee on von Willebrand Factor. J Thromb Haemost. 2006;4:2103–14. - PubMed
-
- Batlle J, Perez-Rodriguez A, Franqueira MD, Lopez-Fernandez MF. Type 2M von Willebrand disease: a variant of type 2A? J Thromb Haemost. 2008;6:388–90. - PubMed
-
- Eikenboom JC, Matsushita T, Reitsma PH, Tuley EA, Castaman G, Briet E, et al. Dominant type 1 von Willebrand disease caused by mutated cysteine residues in the D3 domain of von Willebrand factor. Blood. 1996;88:2433–41. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
